


 Control
Control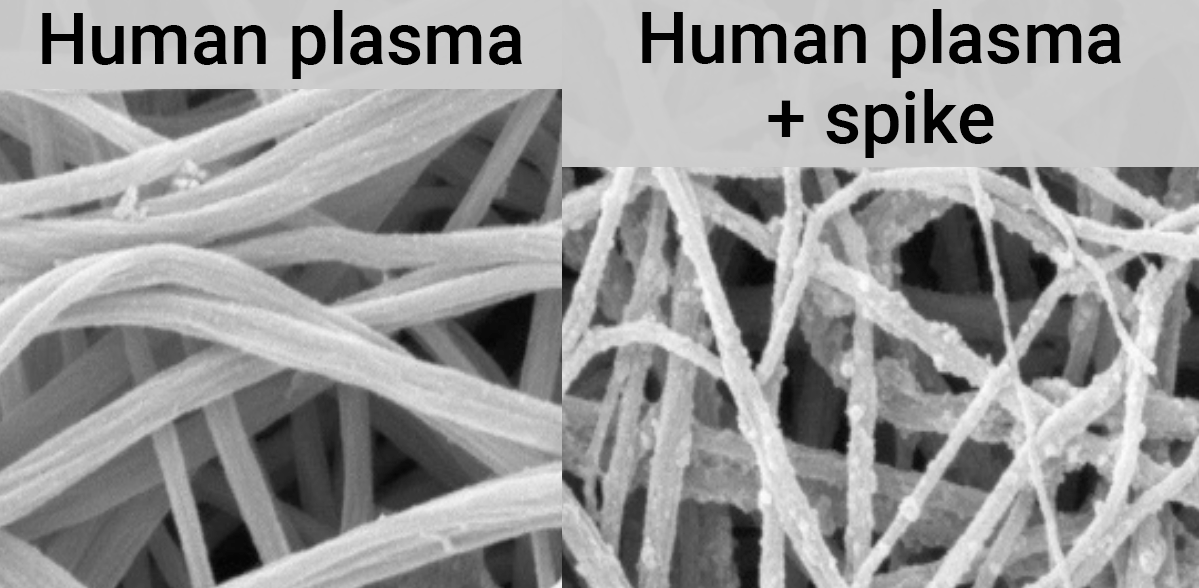
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
We use fixed pre-specified effect extraction to avoid bias and to focus on the
most clinically relevant results. For comparison, we have also performed
analysis using the primary outcome of studies (shown in the
supplementary data),
with results showing similar effect sizes. Prophylaxis results are
very similar with 100% (17 of 17) positive effects. Early
treatment shows 85% (34 of 40) positive effects, improved due
to the very small event count negative serious outcomes in Krolewiecki,
Vallejos, and Buonfrate no longer having priority. Late treatment shows
71% (34 of 48) positive effects, reduced slightly, primarily
due to viral clearance results being the primary outcome in some studies, and
viral clearance being less successful with late treatment. Overall, the
primary outcome analysis shows 81% (85 of 105) positive
effects,
which is currently identical to the results of the main protocol analysis.
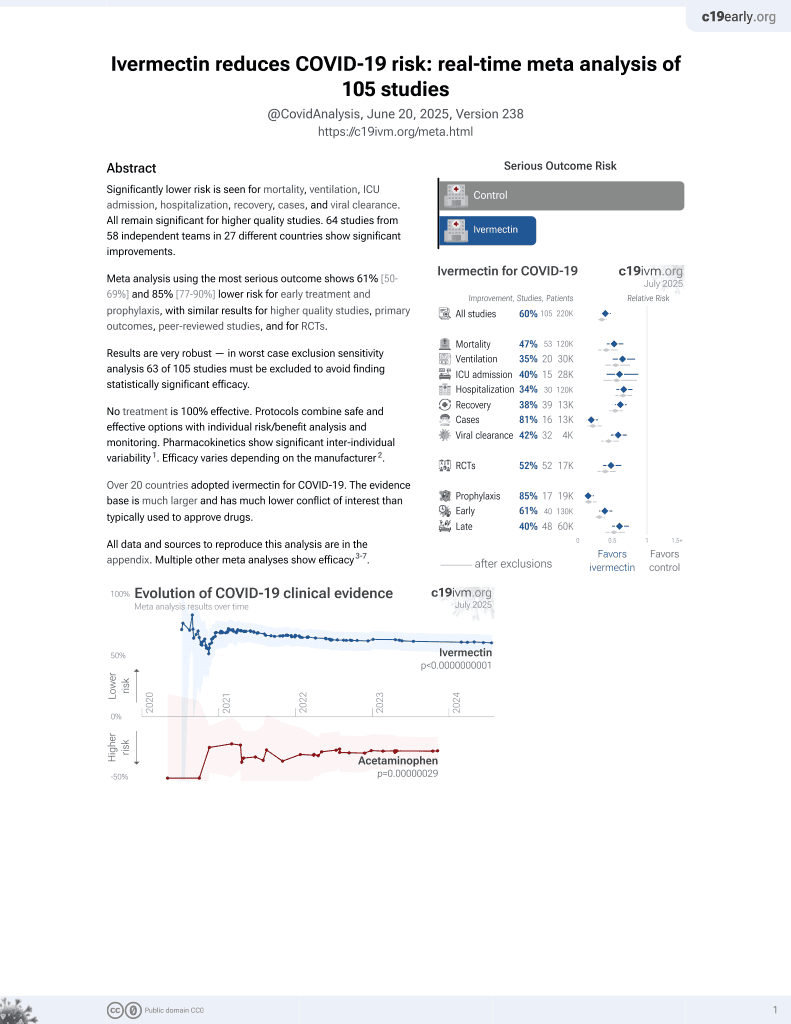
Ivermectin reduces COVID-19 risk: real-time meta analysis of 105 studies
Abstract
Significantly lower risk is seen for mortality, ventilation, ICU admission, hospitalization, recovery, cases, and viral clearance.
All remain significant for higher quality studies.
64 studies
from 58 independent teams
in 27 different countries
show significant improvements.
Meta analysis using the most serious
outcome shows 61% [50‑69%] and 85% [77‑90%] lower risk for early
treatment and prophylaxis, with similar results for
higher quality studies,
primary outcomes, peer-reviewed studies, and for
RCTs.
Results are very robust — in
worst case exclusion sensitivity analysis 63 of 105 studies must be
excluded to avoid finding statistically significant efficacy.
No treatment is 100%
effective. Protocols combine safe and effective options with individual
risk/benefit analysis and monitoring.
Pharmacokinetics show significant inter-individual variability1.
Efficacy varies depending on the manufacturer2.
Over 20 countries adopted ivermectin
for COVID-19. The evidence base is much larger and has much lower conflict of
interest than typically used to approve drugs.
Ivermectin for COVID-19 — Highlights
Ivermectin reduces risk with very high confidence for mortality, ventilation, ICU admission, hospitalization, progression, recovery, cases, viral clearance, and in pooled analysis.
Early treatment and prophylaxis are more effective than late treatment.
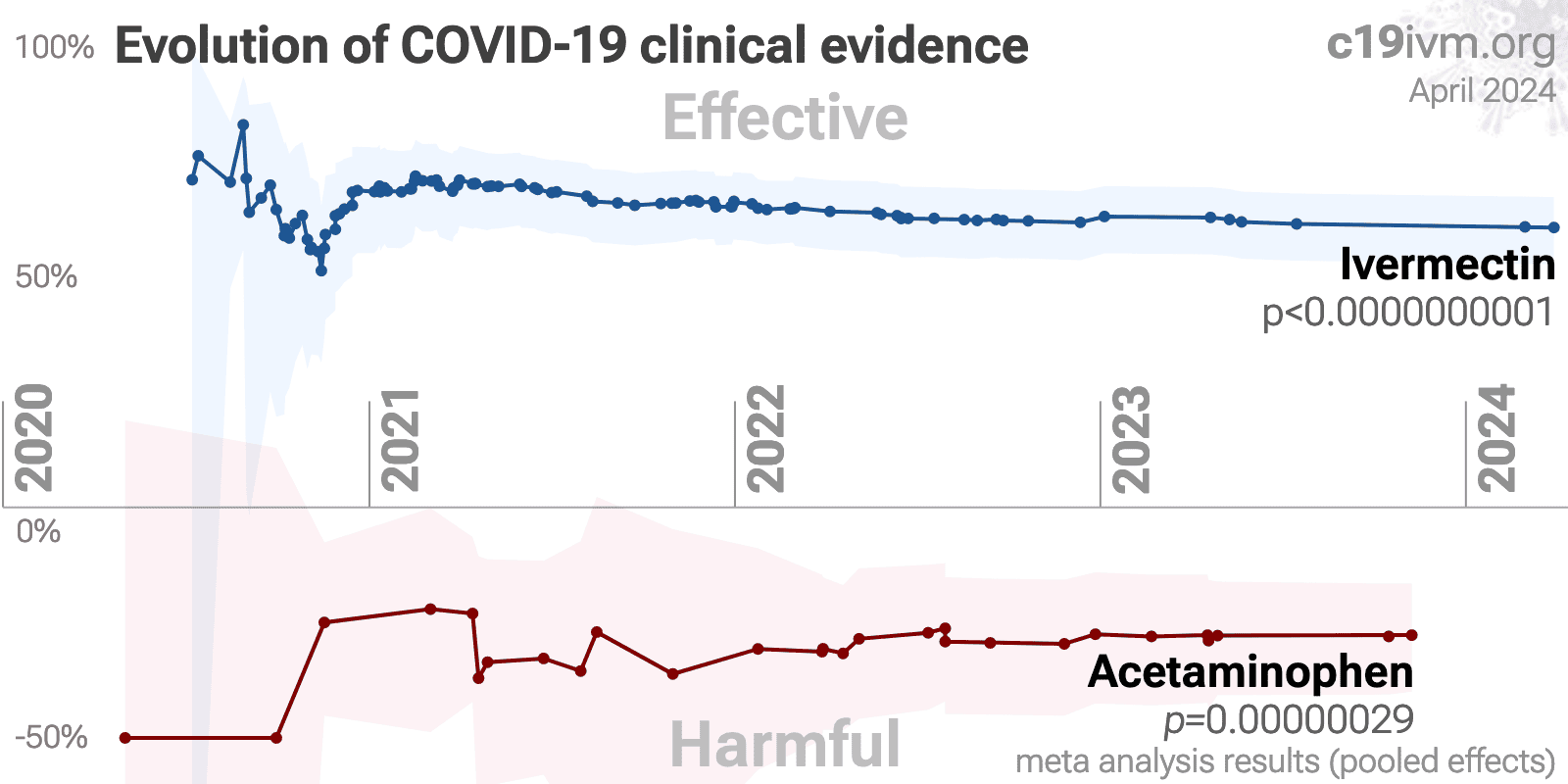
4th treatment shown effective in August 2020, now with p < 0.00000000001 from 105 studies, recognized in 24 countries.
Real-time updates and corrections with a consistent protocol for 172 treatments. Outcome specific analysis and combined evidence from all studies including treatment delay, a primary confounding factor.
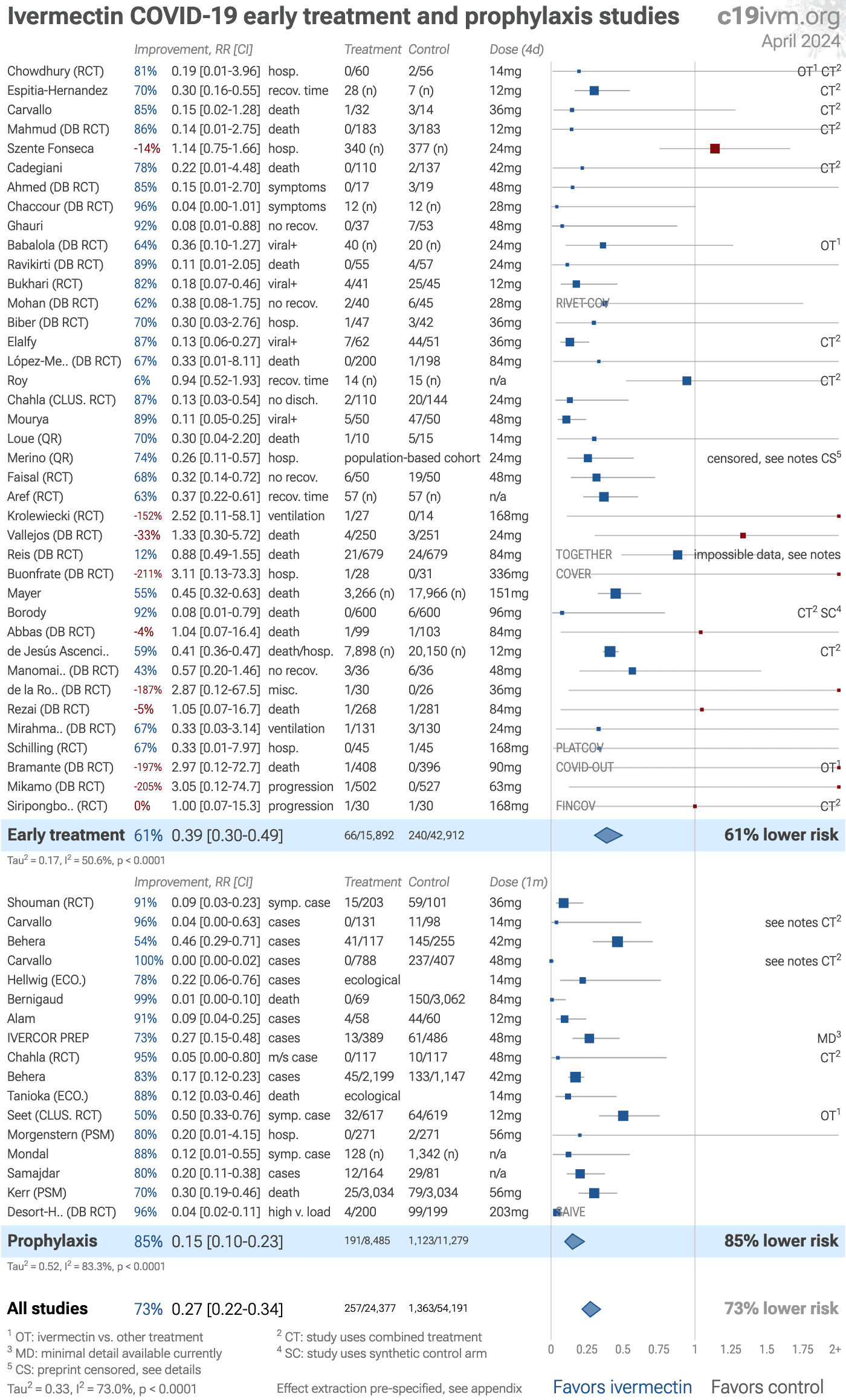
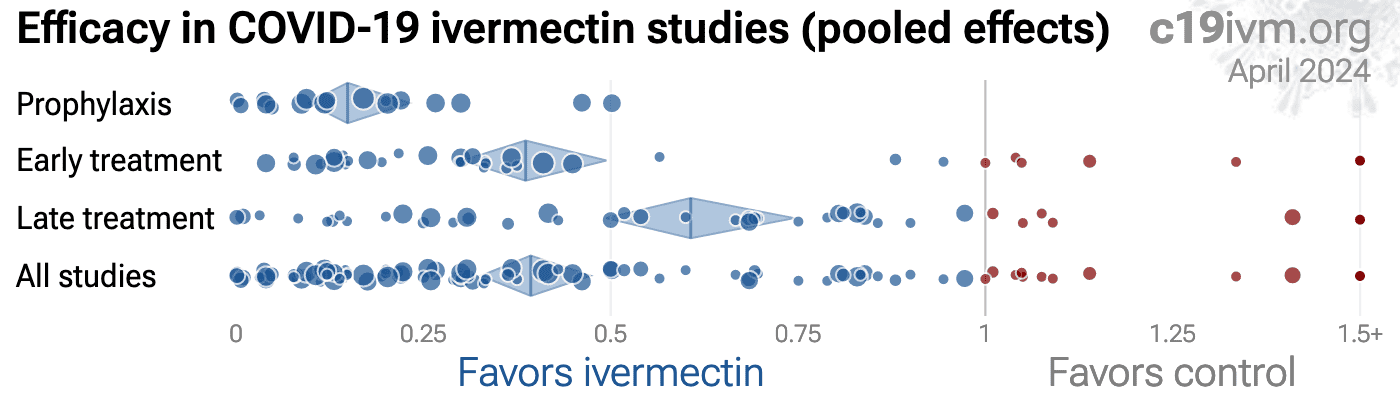
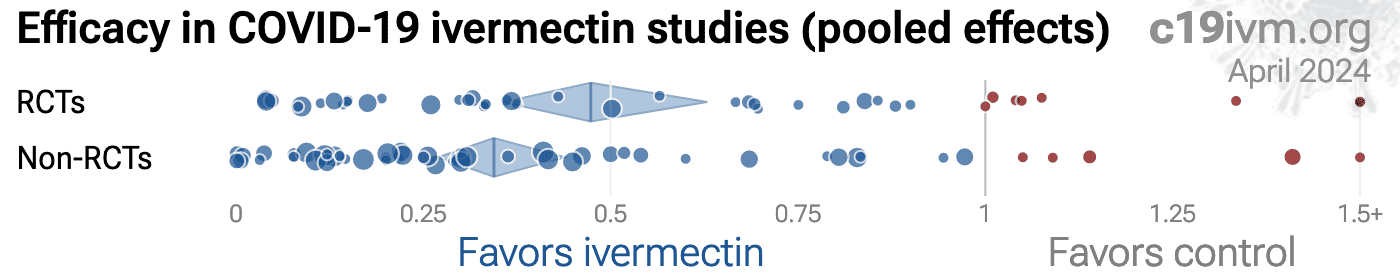
Figure 1.
A. Random effects meta-analysis excluding late treatment. This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first four days for treatment, or the monthly dose for prophylaxis, for a
70kg person. For details of effect extraction and full dosage information
see the appendix.
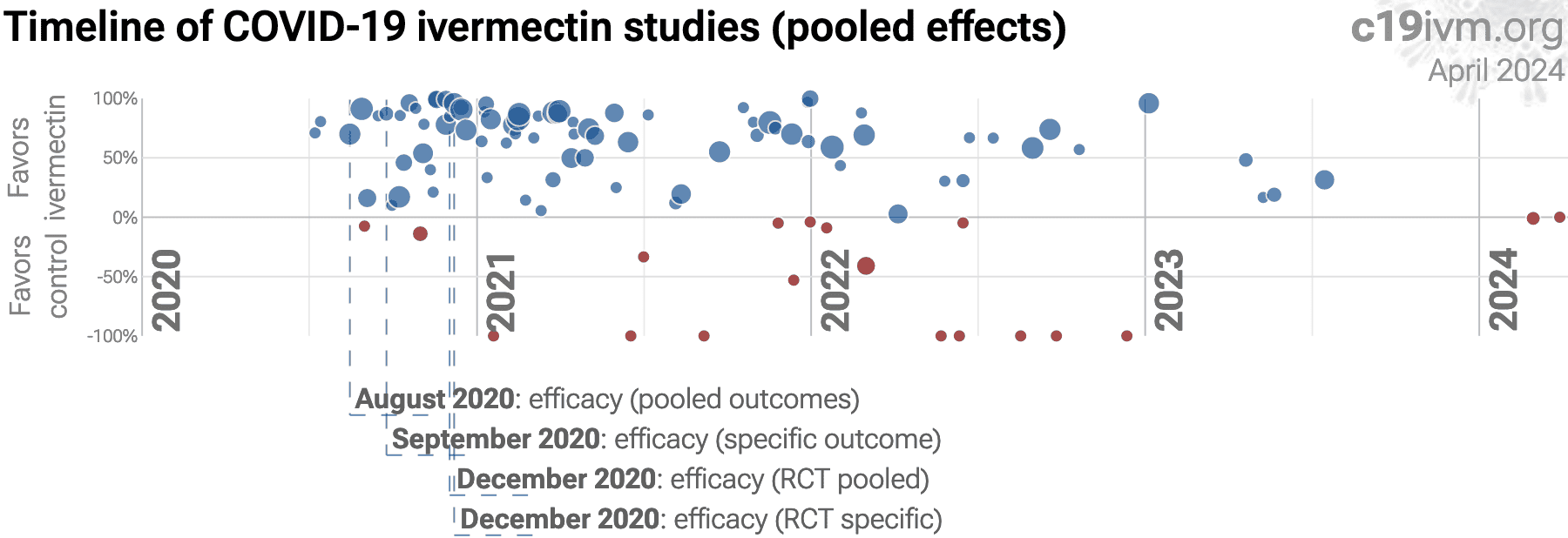
B. Timeline of results in ivermectin studies. The marked dates indicate the time when efficacy was known with a statistically significant improvement of ≥10% from ≥3 studies for pooled outcomes, one or more specific outcome, pooled outcomes in RCTs, and one or more specific outcome in RCTs. Efficacy based on RCTs only was delayed by 3.6 months, compared to using all studies. Efficacy based on specific outcomes was delayed by 1.3 months, compared to using pooled outcomes.
SARS-CoV-2 infection primarily begins in the upper respiratory
tract and may progress to the lower respiratory tract, other tissues, and the
nervous and cardiovascular systems, which may lead to cytokine storm,
pneumonia, ARDS, neurological injury9-21 and
cognitive deficits12,17, cardiovascular
complications22-26, organ failure, and death.
Even mild untreated infections may result in persistent cognitive
deficits27—the spike protein binds to fibrin leading to
fibrinolysis-resistant blood clots, thromboinflammation, and
neuropathology.
Minimizing replication as early as possible is recommended.
SARS-CoV-2 infection and replication involves the complex interplay of 100+
host and viral proteins and other factorsA,28-35, providing many
therapeutic targets for which many existing compounds have known activity.
Scientists have predicted that over 9,000 compounds may
reduce COVID-19 risk36, either by
directly minimizing infection or replication, by supporting immune system
function, or by minimizing secondary complications.
Ivermectin, better known for antiparasitic activity, is a broad spectrum antiviral with activity against many viruses including H7N737, Dengue38-40, HIV-139, Simian virus 4041, Zika40,42,43 , West Nile43, Yellow Fever44,45, Japanese encephalitis44, Chikungunya45, Semliki Forest virus45, Human papillomavirus46, Epstein-Barr46, BK Polyomavirus47, and Sindbis virus45.
Ivermectin inhibits importin-α/β-dependent nuclear import of viral proteins37,39,41,48 , shows spike-ACE2 disruption at 1nM with microfluidic diffusional sizing49, binds to glycan sites on the SARS-CoV-2 spike protein preventing interaction with blood and epithelial cells and inhibiting hemagglutination50,51, shows dose-dependent inhibition of wildtype and omicron variants52, exhibits dose-dependent inhibition of lung injury53,54, may inhibit SARS-CoV-2 via IMPase inhibition40, may inhibit SARS-CoV-2 induced formation of fibrin clots resistant to degradation55, inhibits SARS-CoV-2 3CLpro56, may inhibit SARS-CoV-2 RdRp activity57, may minimize viral myocarditis by inhibiting NF-κB/p65-mediated inflammation in macrophages58, may be beneficial for COVID-19 ARDS by blocking GSDMD and NET formation59, may interfere with SARS-CoV-2's immune evasion via ORF8 binding60, may inhibit SARS-CoV-2 by disrupting CD147 interaction61-64, shows protection against inflammation, cytokine storm, and mortality in an LPS mouse model sharing key pathological features of severe COVID-1965,66, may be beneficial in severe COVID-19 by binding IGF1 to inhibit the promotion of inflammation, fibrosis, and cell proliferation that leads to lung damage67, may minimize SARS-CoV-2 induced cardiac damage68,69, may counter immune evasion by inhibiting NSP15-TBK1/KPNA1 interaction and restoring IRF3 activation70, may disrupt SARS-CoV-2 N and ORF6 protein nuclear transport and their suppression of host interferon responses71, reduces TAZ/YAP nuclear import, relieving SARS-CoV-2-driven suppression of IRF3 and NF-κB antiviral pathways72, increases Bifidobacteria which play a key role in the immune system73, has immunomodulatory74 and anti-inflammatory75,76 properties, and has an extensive and very positive safety profile77.
We analyze all significant controlled studies of ivermectin for
COVID-19. Search methods, inclusion criteria, effect extraction criteria (more
serious outcomes have priority), all individual study data, PRISMA answers,
and statistical methods are detailed in Appendix 1. We present random
effects meta-analysis results for all studies, studies within each treatment
stage, mortality, ventilation, ICU admission, hospitalization, recovery,
cases, viral clearance, peer-reviewed studies, Randomized Controlled Trials
(RCTs), and after exclusion of lower quality studies.
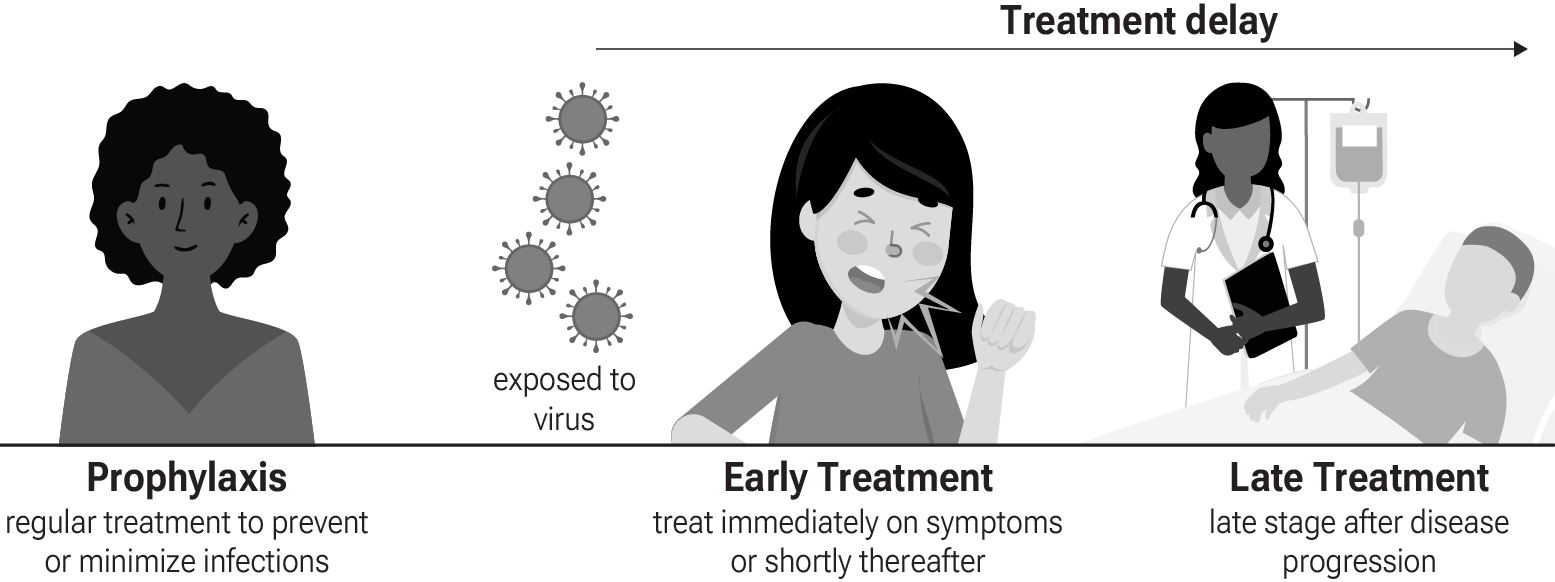
Figure 3 shows stages of possible treatment for
COVID-19. Prophylaxis refers to regularly taking medication before
becoming sick, in order to prevent or minimize infection. Early
Treatment refers to treatment immediately or soon after symptoms appear,
while Late Treatment refers to more delayed treatment.
Figure 3. Treatment stages.
Ivermectin, better known for antiparasitic activity, is a broad spectrum antiviral with activity against many viruses including H7N737, Dengue38-40, HIV-139, Simian virus 4041, Zika40,42,43 , West Nile43, Yellow Fever44,45, Japanese encephalitis44, Chikungunya45, Semliki Forest virus45, Human papillomavirus46, Epstein-Barr46, BK Polyomavirus47, and Sindbis virus45.
Ivermectin inhibits importin-α/β-dependent nuclear import of viral proteins37,39,41,48 , shows spike-ACE2 disruption at 1nM with microfluidic diffusional sizing49, binds to glycan sites on the SARS-CoV-2 spike protein preventing interaction with blood and epithelial cells and inhibiting hemagglutination50,51, shows dose-dependent inhibition of wildtype and omicron variants52, exhibits dose-dependent inhibition of lung injury53,54, may inhibit SARS-CoV-2 via IMPase inhibition40, may inhibit SARS-CoV-2 induced formation of fibrin clots resistant to degradation55, inhibits SARS-CoV-2 3CLpro56, may inhibit SARS-CoV-2 RdRp activity57, may minimize viral myocarditis by inhibiting NF-κB/p65-mediated inflammation in macrophages58, may be beneficial for COVID-19 ARDS by blocking GSDMD and NET formation59, may interfere with SARS-CoV-2's immune evasion via ORF8 binding60, may inhibit SARS-CoV-2 by disrupting CD147 interaction61-64, shows protection against inflammation, cytokine storm, and mortality in an LPS mouse model sharing key pathological features of severe COVID-1965,66, may be beneficial in severe COVID-19 by binding IGF1 to inhibit the promotion of inflammation, fibrosis, and cell proliferation that leads to lung damage67, may minimize SARS-CoV-2 induced cardiac damage68,69, may counter immune evasion by inhibiting NSP15-TBK1/KPNA1 interaction and restoring IRF3 activation70, may disrupt SARS-CoV-2 N and ORF6 protein nuclear transport and their suppression of host interferon responses71, and reduces TAZ/YAP nuclear import, relieving SARS-CoV-2-driven suppression of IRF3 and NF-κB antiviral pathways72.
7 studies investigate novel formulations of ivermectin that may be more
effective for COVID-19109,122,123,127-130 .
Preclinical research is an important part of the development of
treatments, however results may be very different in clinical trials.
Preclinical results are not used in this paper.
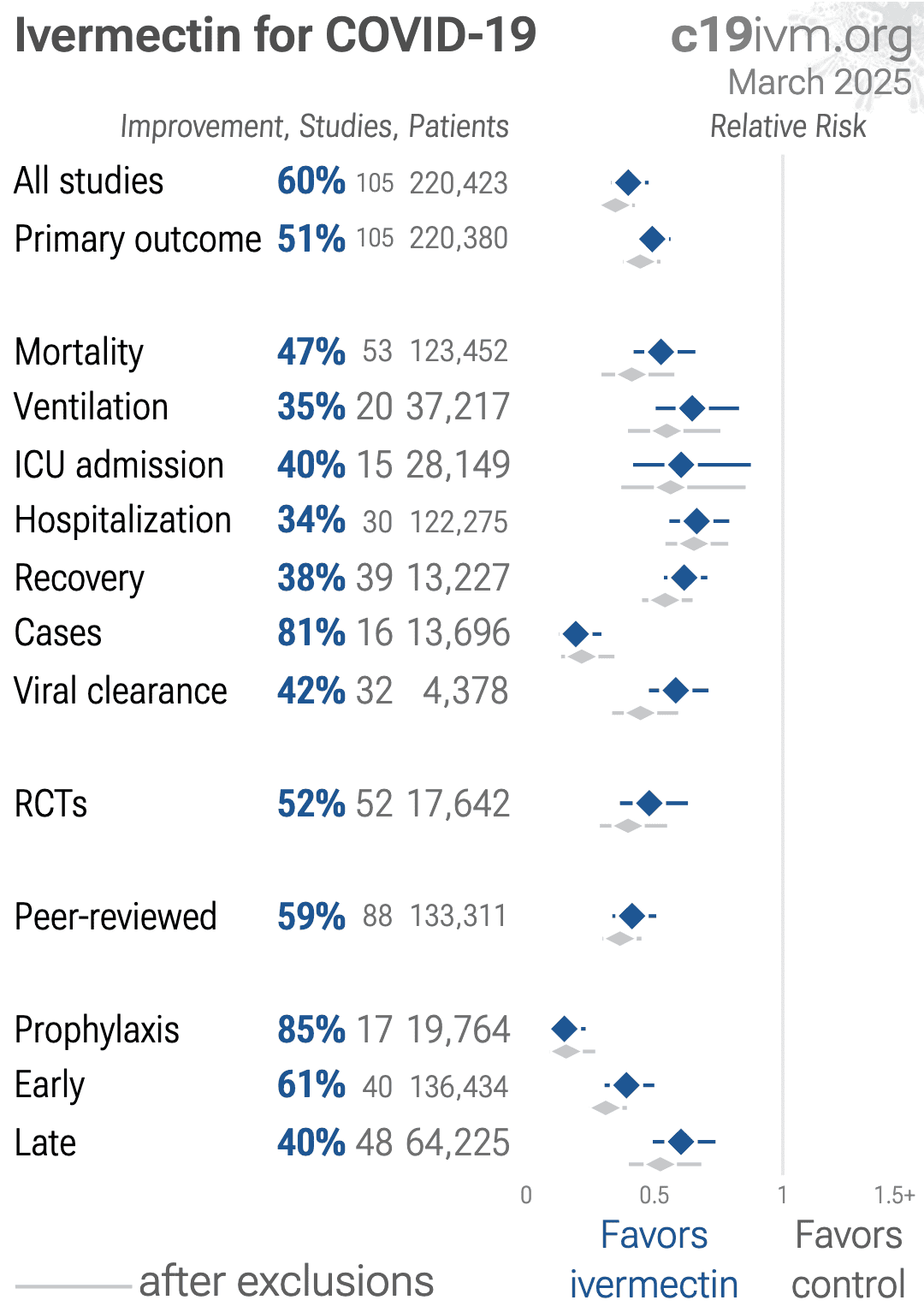
Table 1 summarizes the results of random-effects meta analysis for all stages combined, for Randomized Controlled Trials, for peer-reviewed studies, with different exclusions, and for specific outcomes.
Table 2 shows results by treatment stage.
Figure 4 plots individual results by treatment stage.
Figure 5, 6, 7, 8, 9, 10, 11, and 12
show forest plots for random effects meta-analysis of all studies with pooled
effects, and for specific outcomes: mortality, ICU admission, mechanical
ventilation, hospitalization, recovery, cases, and viral clearance.
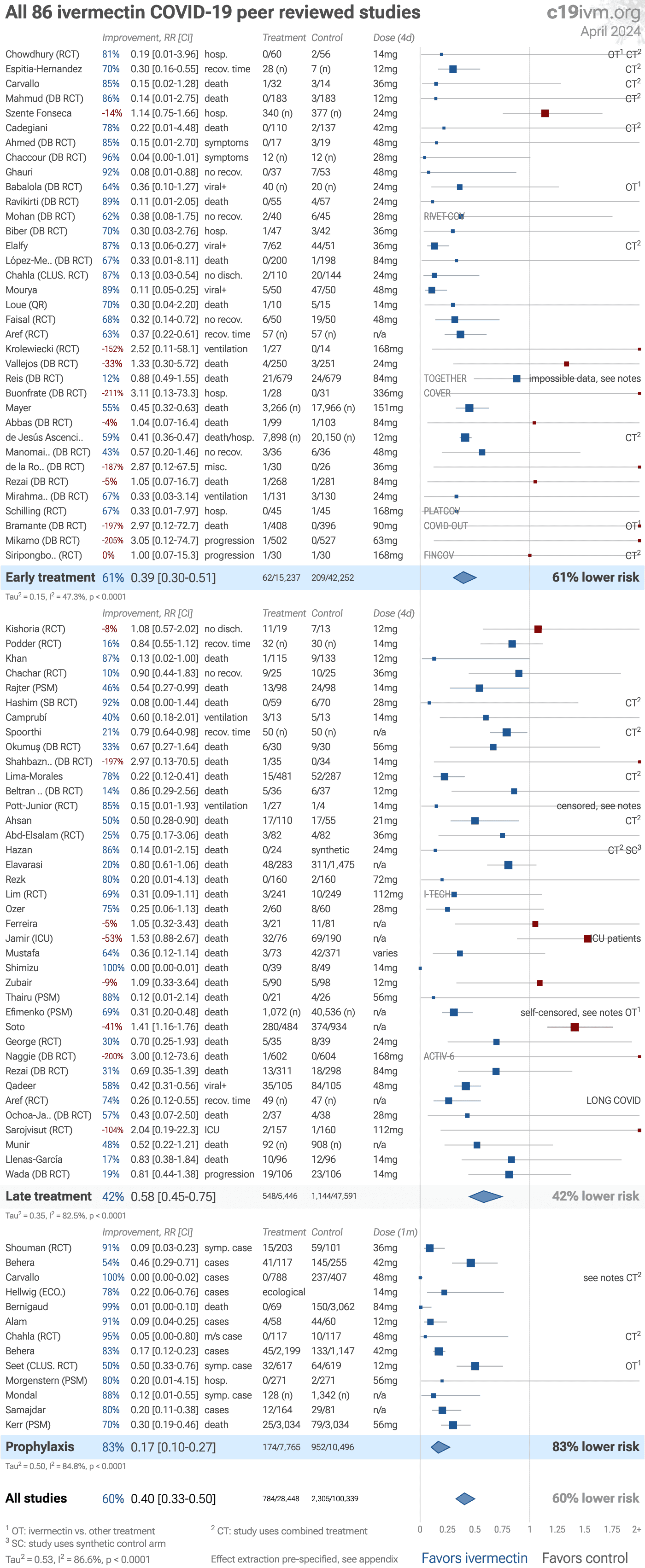
Figure 13 shows results for peer reviewed trials only, and the
supplementary data contains peer reviewed and individual outcome results after
exclusions.
| Relative Risk | Studies | Patients | |
|---|---|---|---|
| All studies | 0.40 [0.33‑0.48] p < 0.0001**** | 105 | 220K |
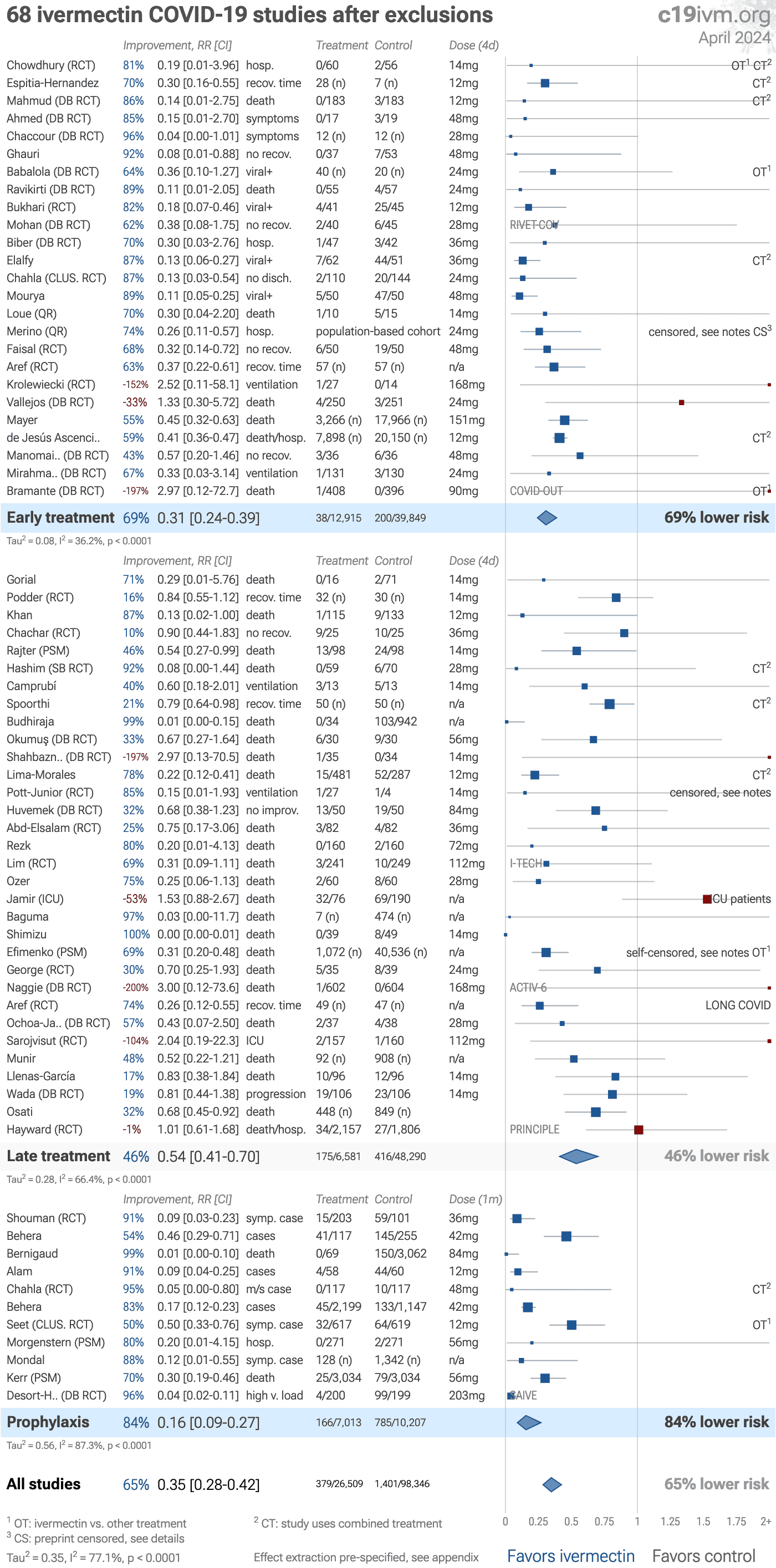
| After exclusions | 0.35 [0.28‑0.42] p < 0.0001**** | 70 | 200K |
| Peer-reviewedPeer-reviewed | 0.41 [0.34‑0.51] p < 0.0001**** | 88 | 130K |
| RCTsRCTs | 0.48 [0.37‑0.63] p < 0.0001**** | 52 | 10K |
| RCTs after exclusionsRCTs w/exc. | 0.40 [0.29‑0.55] p < 0.0001**** | 39 | 10K |
| Mortality | 0.53 [0.42‑0.66] p < 0.0001**** | 53 | 120K |
| VentilationVent. | 0.65 [0.50‑0.83] p = 0.00063*** | 20 | 30K |
| ICU admissionICU | 0.60 [0.42‑0.88] p = 0.0078** | 15 | 20K |
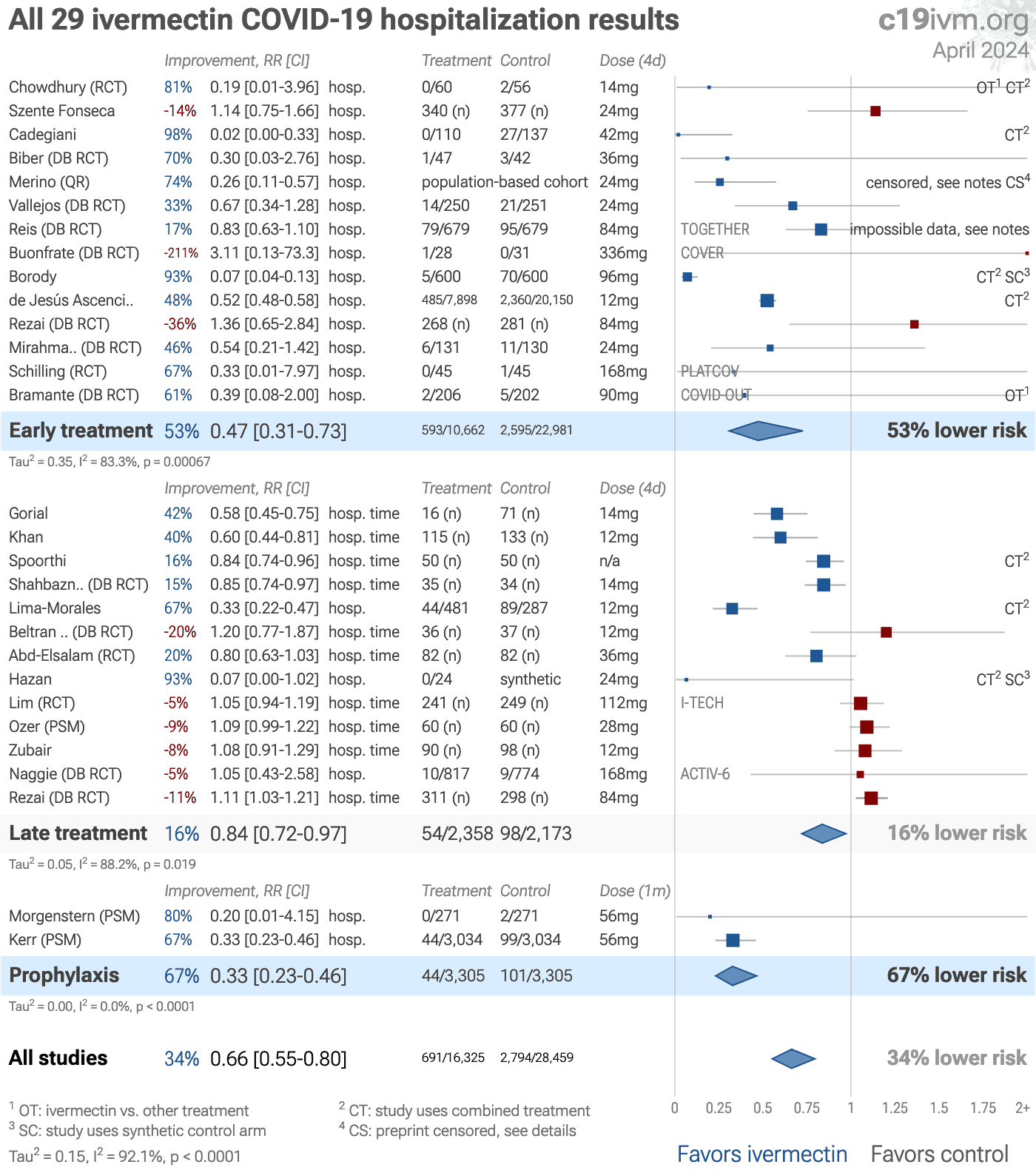
| HospitalizationHosp. | 0.66 [0.56‑0.79] p < 0.0001**** | 30 | 120K |
| Recovery | 0.62 [0.54‑0.71] p < 0.0001**** | 39 | 10K |
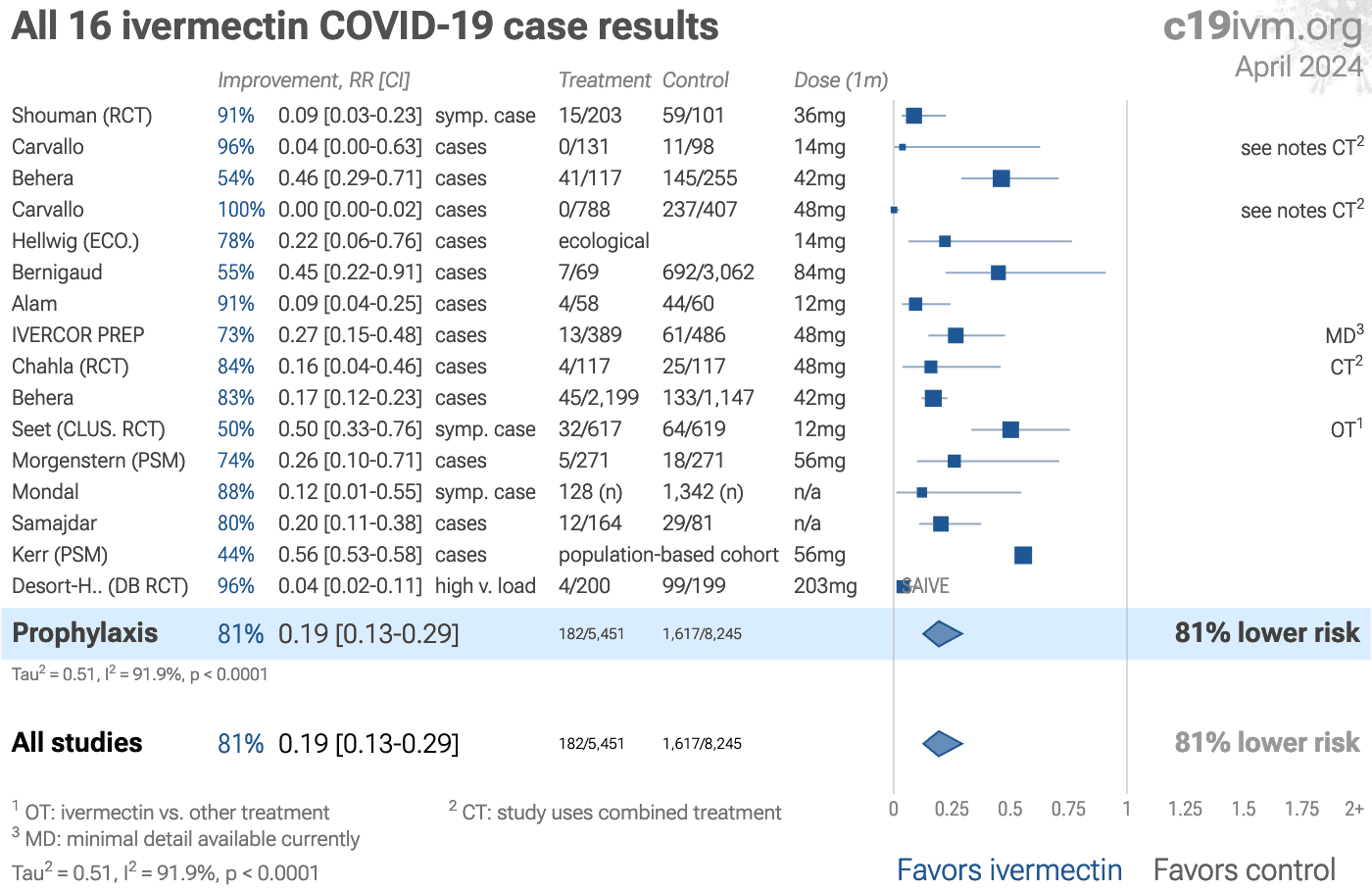
| Cases | 0.19 [0.13‑0.29] p < 0.0001**** | 16 | 10K |
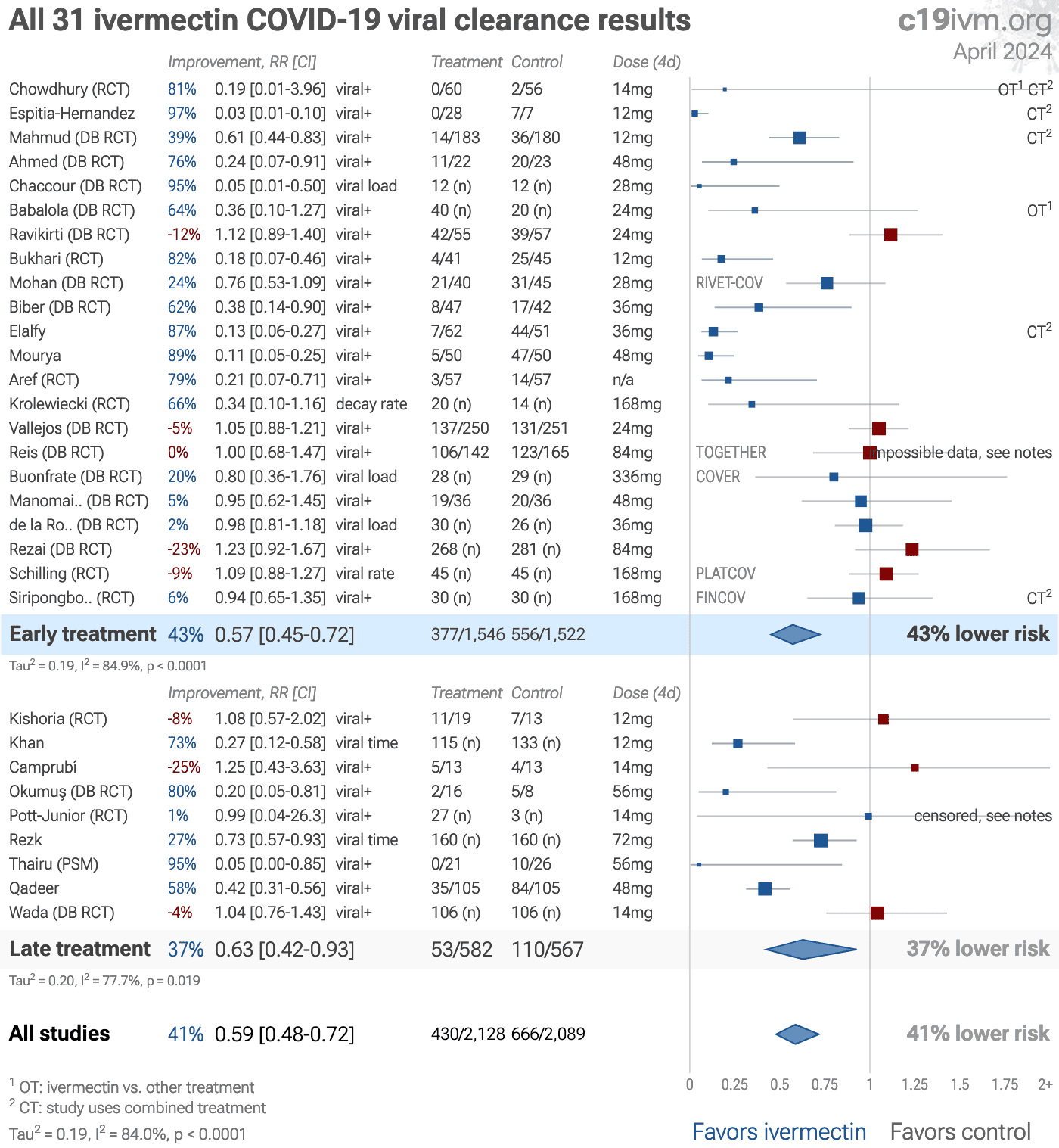
| Viral | 0.58 [0.48‑0.71] p < 0.0001**** | 32 | 4,378 |
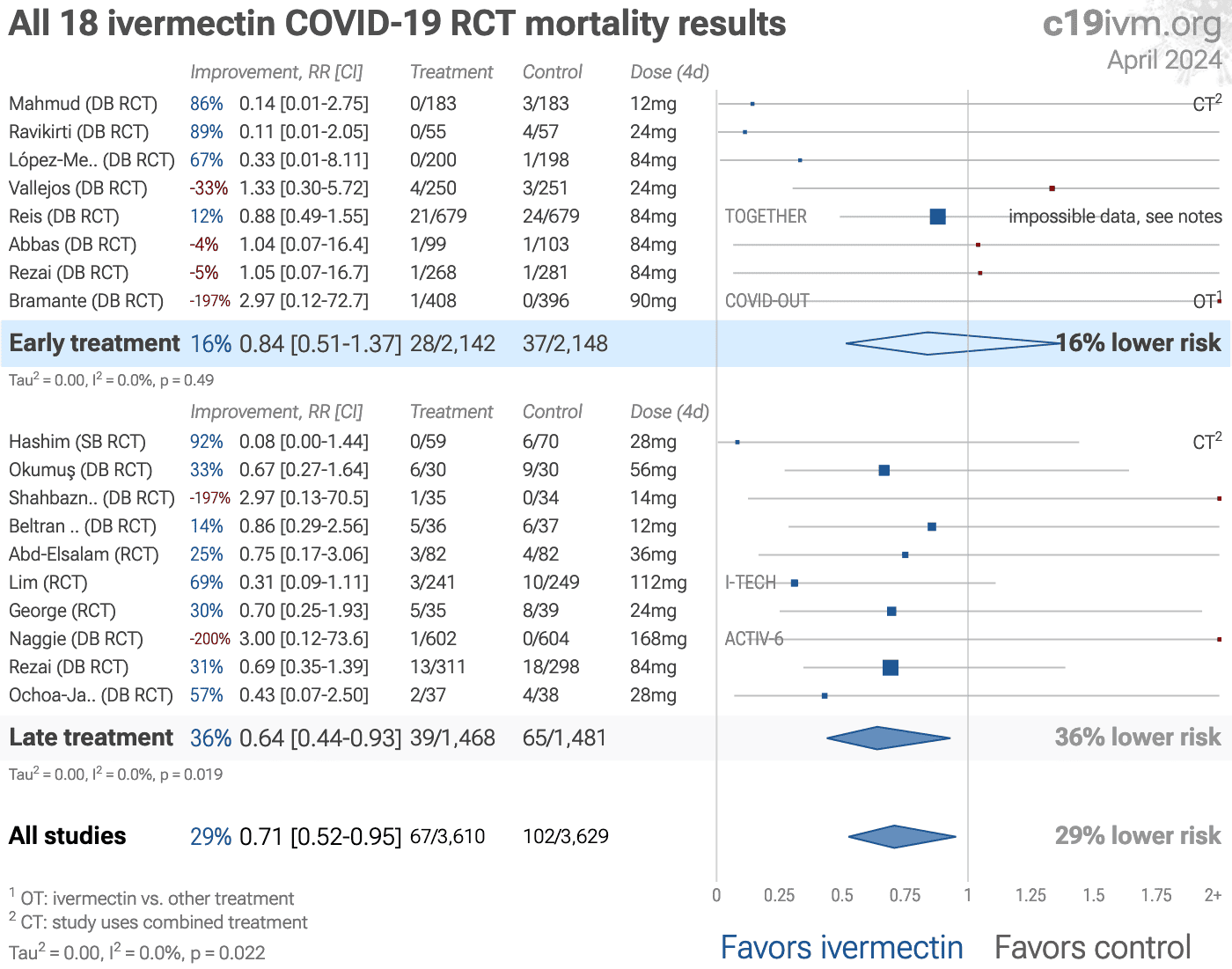
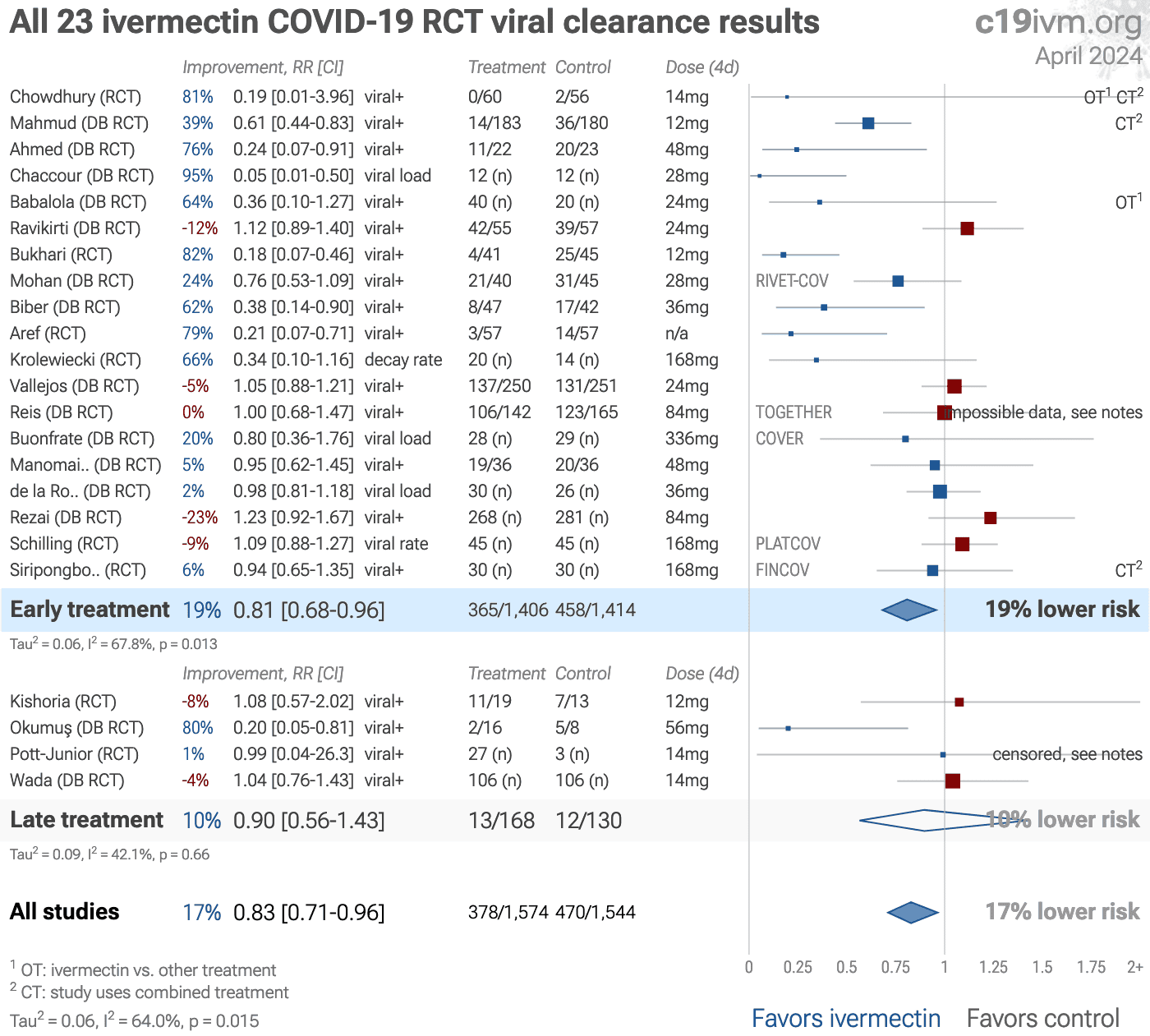
| RCT mortality | 0.74 [0.56‑0.97] p = 0.027* | 20 | 7,864 |
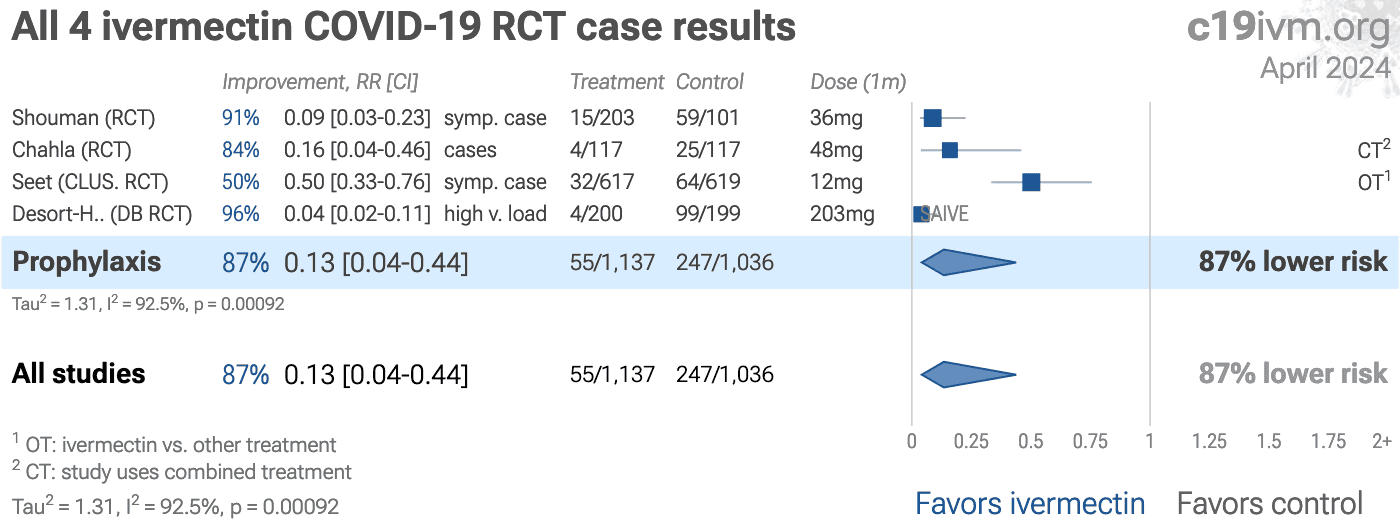
| RCT casesRCT cases | 0.13 [0.04‑0.44] p = 0.00092*** | 4 | 2,173 |
| RCT viral | 0.81 [0.69‑0.94] p = 0.0064** | 24 | 3,279 |
| Early treatment | Late treatment | Prophylaxis | |
|---|---|---|---|
| All studies | 0.39 [0.31‑0.50]****0.39**** [0.31‑0.50] | 0.60 [0.49‑0.74]****0.60**** [0.49‑0.74] | 0.15 [0.10‑0.23]****0.15**** [0.10‑0.23] |
| After exclusions | 0.31 [0.24‑0.39]****0.31**** [0.24‑0.39] | 0.52 [0.40‑0.68]****0.52**** [0.40‑0.68] | 0.16 [0.09‑0.27]****0.16**** [0.09‑0.27] |
| Peer-reviewedPeer-reviewed | 0.40 [0.31‑0.52]****0.40**** [0.31‑0.52] | 0.59 [0.46‑0.75]****0.59**** [0.46‑0.75] | 0.17 [0.10‑0.27]****0.17**** [0.10‑0.27] |
| RCTsRCTs | 0.45 [0.33‑0.61]****0.45**** [0.33‑0.61] | 0.72 [0.59‑0.88]**0.72** [0.59‑0.88] | 0.11 [0.03‑0.43]**0.11** [0.03‑0.43] |
| RCTs after exclusionsRCTs w/exc. | 0.35 [0.26‑0.47]****0.35**** [0.26‑0.47] | 0.66 [0.50‑0.86]**0.66** [0.50‑0.86] | 0.11 [0.03‑0.43]**0.11** [0.03‑0.43] |
| Mortality | 0.61 [0.42‑0.89]*0.61* [0.42‑0.89] | 0.57 [0.44‑0.74]****0.57**** [0.44‑0.74] | 0.10 [0.02‑0.50]**0.10** [0.02‑0.50] |
| VentilationVent. | 0.81 [0.56‑1.16]0.81 [0.56‑1.16] | 0.53 [0.39‑0.72]****0.53**** [0.39‑0.72] | |
| ICU admissionICU | 0.48 [0.24‑0.97]*0.48* [0.24‑0.97] | 0.65 [0.43‑0.98]*0.65* [0.43‑0.98] | |
| HospitalizationHosp. | 0.47 [0.31‑0.73]***0.47*** [0.31‑0.73] | 0.82 [0.71‑0.95]**0.82** [0.71‑0.95] | 0.33 [0.23‑0.46]****0.33**** [0.23‑0.46] |
| Recovery | 0.45 [0.31‑0.66]****0.45**** [0.31‑0.66] | 0.73 [0.65‑0.83]****0.73**** [0.65‑0.83] | |
| Cases | 0.19 [0.13‑0.29]****0.19**** [0.13‑0.29] |
||
| Viral | 0.57 [0.45‑0.71]****0.57**** [0.45‑0.71] | 0.63 [0.42‑0.93]*0.63* [0.42‑0.93] | |
| RCT mortality | 0.86 [0.53‑1.40]0.86 [0.53‑1.40] | 0.69 [0.50‑0.95]*0.69* [0.50‑0.95] | |
| RCT casesRCT cases | 0.13 [0.04‑0.44]***0.13*** [0.04‑0.44] |
||
| RCT viral | 0.79 [0.66‑0.93]**0.79** [0.66‑0.93] | 0.90 [0.56‑1.43]0.90 [0.56‑1.43] | |
Figure 4. Results by treatment stage.
Loading..
Loading..
Figure 5. Random effects meta-analysis for all studies. This plot shows pooled effects,
see the specific outcome analyses for individual outcomes.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Effect extraction is pre-specified, using the most serious outcome reported.
Simplified dosages are shown for comparison, these are the total dose in the
first four days for treatment, or the monthly dose for prophylaxis, for a
70kg person. For details of effect extraction and full dosage information
see the appendix.
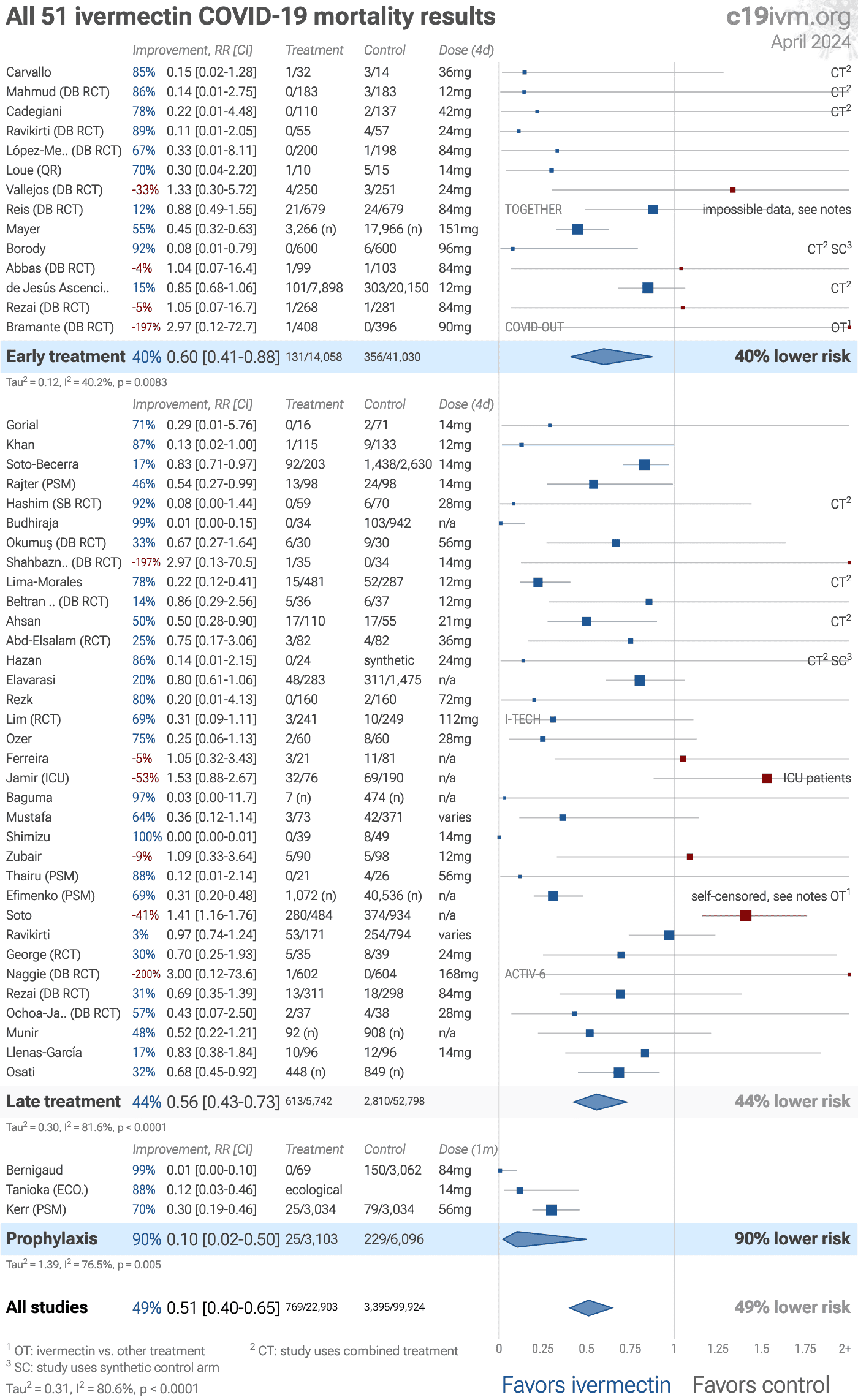
Figure 6.
Random effects meta-analysis for mortality.
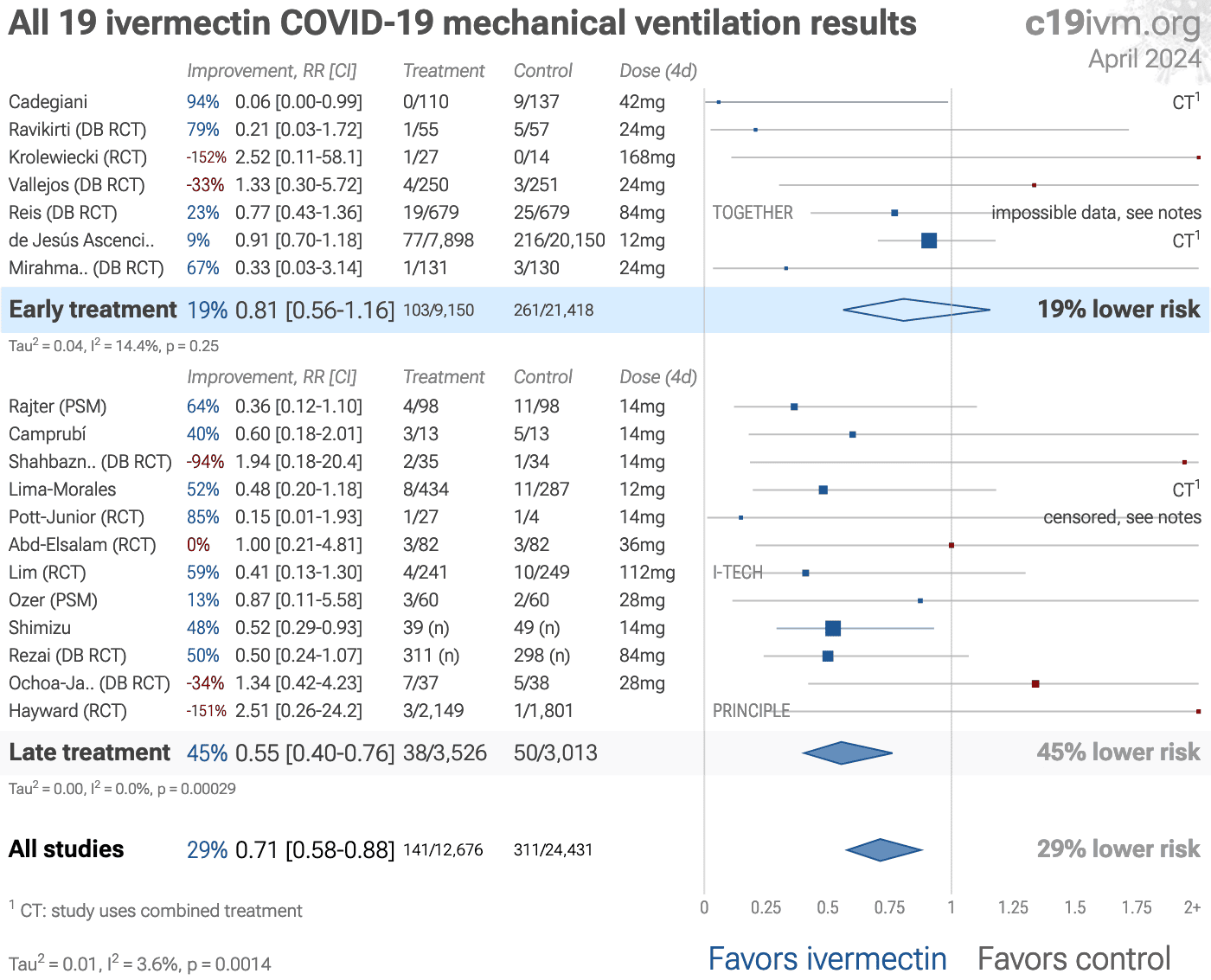
Figure 7. Random effects meta-analysis for
mechanical ventilation.
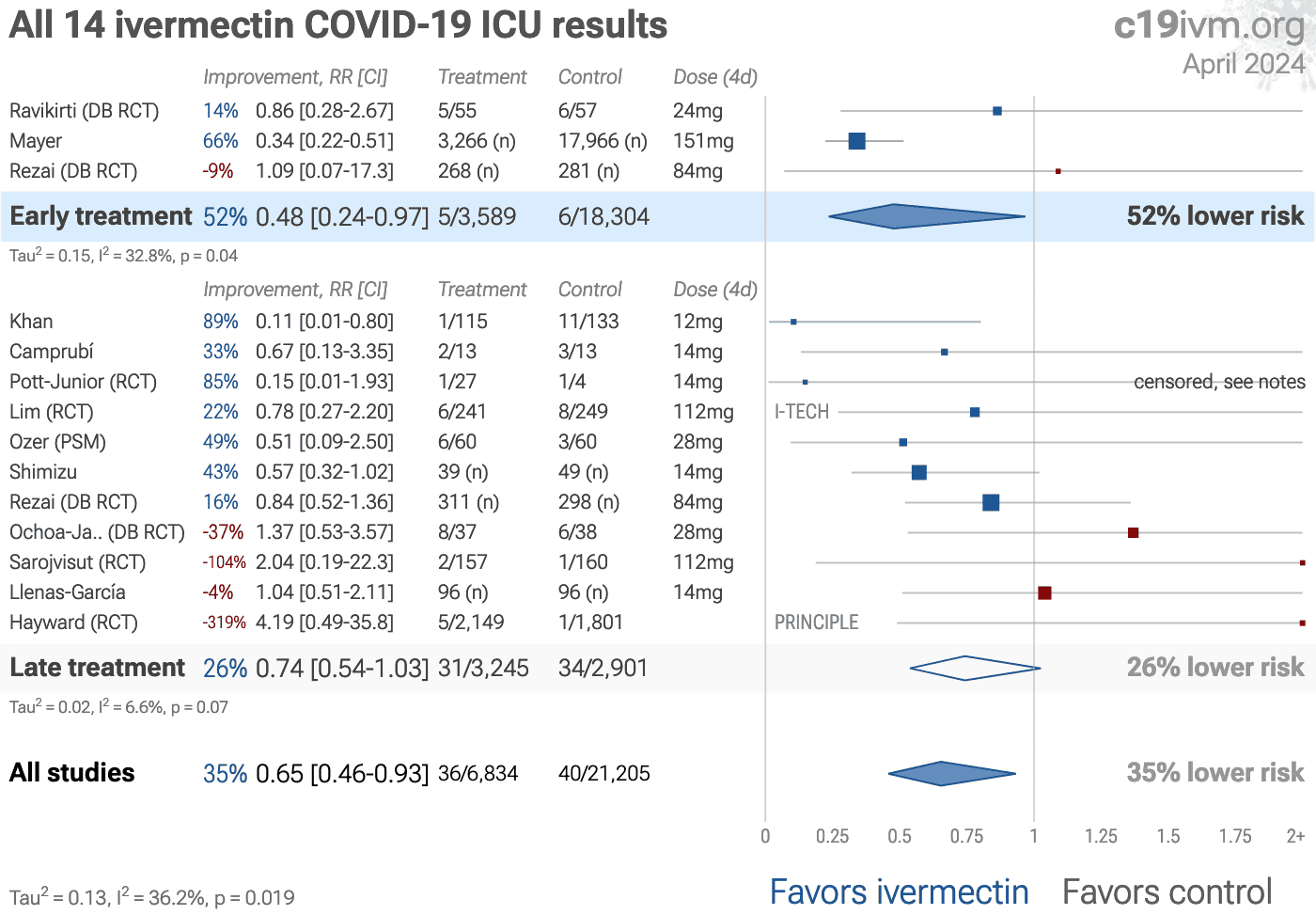
Figure 8. Random effects meta-analysis for
ICU admission.
Figure 9. Random effects meta-analysis for
hospitalization.
Figure 10. Random effects meta-analysis for
recovery results only.
Figure 11. Random effects meta-analysis for
COVID-19 case results.
Figure 12. Random effects meta-analysis for
viral clearance.
Figure 13. Random effects meta-analysis for
peer-reviewed trials.
Zeraatkar et al. analyze 356 COVID-19 trials, finding no significant
evidence that preprint results are inconsistent with peer-reviewed studies.
They also show extremely long peer-review delays, with a median of 6 months to
journal publication. A six month delay was equivalent to around 1.5 million
deaths during the first two years of the pandemic. Authors recommend using
preprint evidence, with appropriate checks for potential falsified data, which
provides higher certainty much earlier. Davidson et al. also showed no
important difference between meta analysis results of preprints and
peer-reviewed publications for COVID-19, based on 37 meta analyses including
114 trials.
Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
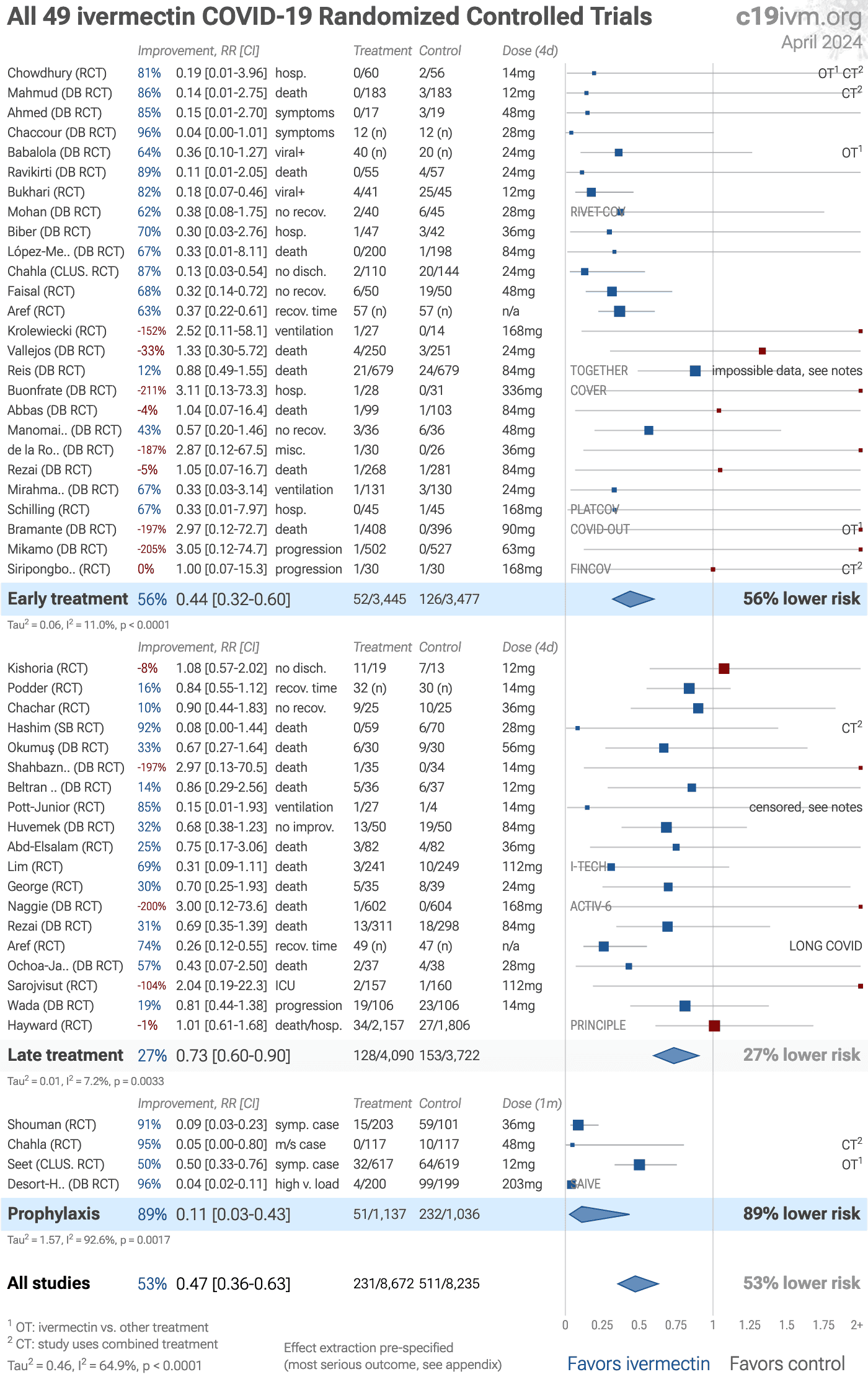
Results restricted to Randomized Controlled Trials (RCTs) are
shown in Figure 14, 15, 16, and 17, Table 1,
and Table 2. The
supplementary data contains RCT results after
exclusions.
Figure 14. Randomized Controlled Trials. The distribution of results for RCTs is similar to the distribution
for all other studies.
Figure 15. Random effects meta-analysis for
Randomized Controlled Trials only. Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
RCTs help to make study groups more similar and can provide a higher level of
evidence, however they are subject to many biases133, and
analysis of double-blind RCTs has identified extreme levels of bias134.
For COVID-19, the overhead may delay treatment, dramatically compromising
efficacy; they may encourage monotherapy for simplicity at the cost of
efficacy which may rely on combined or synergistic effects; the participants
that sign up may not reflect real world usage or the population that benefits
most in terms of age, comorbidities, severity of illness, or other factors;
standard of care may be compromised and unable to evolve quickly based on
emerging research for new diseases; errors may be made in randomization and
medication delivery; and investigators may have hidden agendas or vested
interests influencing design, operation, analysis, reporting, and the
potential for fraud. All of these biases have been observed with COVID-19
RCTs. There is no guarantee that a specific RCT provides a higher level of
evidence.
RCTs are expensive and many RCTs are funded
by pharmaceutical companies or interests closely aligned with pharmaceutical
companies. For COVID-19, this creates an incentive to show efficacy for
patented commercial products, and an incentive to show a lack of efficacy for
inexpensive treatments. The bias is expected to be significant, for example
Als-Nielsen et al. analyzed 370 RCTs from Cochrane reviews, showing that
trials funded by for-profit organizations were 5 times more likely to
recommend the experimental drug compared with those funded by nonprofit
organizations. For COVID-19, some major philanthropic organizations are
largely funded by investments with extreme conflicts of interest for and
against specific COVID-19 interventions.
High quality RCTs for novel acute diseases are more challenging, with
increased ethical issues due to the urgency of treatment, increased risk due
to enrollment delays, and more difficult design with a rapidly evolving
evidence base. For COVID-19, the most common site of initial infection is the
upper respiratory tract. Immediate treatment is likely to be most successful
and may prevent or slow progression to other parts of the body. For a
non-prophylaxis RCT, it makes sense to provide treatment in advance and
instruct patients to use it immediately on symptoms, just as some governments
have done by providing medication kits in advance. Unfortunately, no RCTs have
been done in this way. Every treatment RCT to date involves delayed treatment.
Among the 172 treatments we have analyzed,
67% of RCTs involve very late treatment 5+ days after
onset. No non-prophylaxis COVID-19 RCTs match the potential real-world use of
early treatments. They may more accurately represent results for treatments
that require visiting a medical facility, e.g., those requiring intravenous
administration.
RCTs have a bias against finding an effect for interventions
that are widely available — patients that believe they need the
intervention are more likely to decline participation and take the
intervention. RCTs for ivermectin are more likely to enroll low-risk
participants that do not need treatment to recover, making the results less
applicable to clinical practice. This bias is likely to be greater for widely
known treatments, and may be greater when the risk of a serious outcome is
overstated. This bias does not apply to the typical pharmaceutical trial of a
new drug that is otherwise unavailable.
Figure 19.
For COVID-19, observational study results do not systematically
differ from RCTs, RR 0.98 [0.92‑1.05]
across 172 treatments136.
Evidence shows that observational studies
can also provide reliable results. Concato et al. found that well-designed
observational studies do not systematically overestimate the magnitude of the
effects of treatment compared to RCTs. Anglemyer et al. analyzed reviews
comparing RCTs to observational studies and found little evidence for
significant differences in effect estimates.
We performed a similar analysis across the 172 treatments
we cover, showing no significant difference in the results of RCTs compared to
observational studies, RR 0.98 [0.92‑1.05]139. Similar results are found for all low-cost treatments, RR
1.00 [0.91‑1.09]. High-cost treatments
show a non-significant trend towards RCTs showing greater efficacy,
RR 0.92 [0.84‑1.02].
Details can be found in the
supplementary data.
Lee et al. showed that only 14% of the guidelines of the Infectious
Diseases Society of America were based on RCTs. Evaluation of studies relies
on an understanding of the study and potential biases. Limitations in an RCT
can outweigh the benefits, for example excessive dosages, excessive treatment
delays, or remote survey bias may have a greater effect on results. Ethical
issues may also prevent running RCTs for known effective treatments. For more
on issues with RCTs see141,142.
Currently, 55 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. Of these, 58% have been confirmed in RCTs, with a mean delay of 7.7 months (64% with 8.9 months delay for low-cost treatments). The remaining treatments either have no RCTs, or the point estimate is consistent.
We need to evaluate each trial on its own merits. RCTs for a
given medication and disease may be more reliable, however they may also be
less reliable. For off-patent medications, very high conflict of interest
trials may be more likely to be RCTs, and more likely to be large trials that
dominate meta analyses.
To avoid bias in the selection of studies, we analyze all
non-retracted studies. Here we show the results after excluding studies with
critical issues likely to alter results, non-standard studies, and studies
where very minimal detail is currently available. Our bias evaluation is based
on analysis of each study and identifying when there is a significant chance
that limitations will substantially change the outcome of the study. We
believe this can be more valuable than checklist-based approaches such as
Cochrane GRADE, which may underemphasize serious issues not captured in the
checklists, overemphasize issues unlikely to alter outcomes in specific cases
(for example, lack of blinding for an objective mortality outcome, or certain
specifics of randomization with a very large effect size), or be subject to
bias. However, they can also be very high quality5.
A team of researchers has analyzed the data in ivermectin
studies and identified several studies with concerns. Retracted studies are
not in this analysis. All other studies that the team has identified are
excluded here. For more details see the response
section.
Detailed description of issues with
Reis, Naggie, Bramante, Hayward, López-Medina, Vallejos, Beltran Gonzalez
can be found in the study notes section.
Soto-Becerra is a database analysis covering anyone
with ICD-10 COVID-19 codes, which includes asymptomatic PCR+ patients.
Therefore many patients in the control group are likely asymptomatic with
regards to SARS-CoV-2, but in the hospital for another reason. For those that
had symptomatic COVID-19, there is also likely significant confounding by
indication. KM curves show that the treatment groups were in more serious
condition, with more than the total excess mortality at 30 days occurring on
day 1. All treatments are worse than the control group at 30 days, while at
the latest followup all treatments show lower mortality than control. The
machine learning system used also appears over-parameterized and likely to
result in significant overfitting and inaccurate results. There is also no
real control group in this study - patients receiving the treatments after 48
hours were put in the control group. Authors also state that outcomes within
24 hours were excluded, however the KM curves show significant mortality at
day 1 (only for the treatment groups). Several protocol violations have also
been reported in this study151. Note that this study provides both
30 day mortality and weighted KM curves up to day 43 for ivermectin, we use
the day 43 results as per our protocol. IVERCOR PREP reports prophylaxis
results, however only very minimal details are currently available in a news
report and an online presentation. Hellwig analyze African countries
and COVID-19 cases in October 2020 as a function of whether widespread
prophylactic use of ivermectin is used for parasitic infections.
Tanioka perform a similar analysis for COVID-19 mortality in January
2021. These studies are excluded because they are not clinical trials.
Shahbaznejad had only one death that occurred in a patient that was
critically ill at the time of admission and died within the first 24 hours.
Galan perform an RCT comparing ivermectin and other treatments with
very late stage severe condition hospitalized patients, not showing
significant differences between the treatments. Authors were unable to add a
control arm due to ethical issues. The closest control comparison we could
find is Baqui et al., which shows 43% hospital mortality in the northern
region of Brazil where the study was performed, from which we can estimate the
mortality with ivermectin in this study as 47% lower, RR 0.53. Further, the
study is restricted to more severe cases, hence the expected mortality, and
therefore the benefit of treatment, may be higher. Kishoria restrict
inclusion to patients that did not respond to standard treatment, provide no
details on the time of the discharge status, and there are very large
unadjusted differences in the groups, with over twice as many patients in the
ivermectin group with age >40, and all patients over 60 in the ivermectin
group. Angkasekwinai does not make sense as reported, for details
see160.
Summarizing, the studies excluded are as follows, and the
resulting forest plot is shown in Figure 20.
The
supplementary data shows results after restrictions and exclusions.
Abbas, very minimal patient information, three different results for the recovery outcome, selective omission of the statistically significant recovery p-value, and other inconsistencies.
Ahsan, unadjusted results with no group details.
Beltran Gonzalez, major inconsistencies reported and the data is no longer available163, although the authors state that it is available, and have shared it with an anti-treatment group.
Borody, preliminary report with minimal details.
Buonfrate, significant unadjusted group differences, with 3 times as many patients in the ivermectin arms having the baseline visit in a hospital setting, and arm C having large differences in baseline gender, weight, cough, pyrexia, and anosmia, excessive dose for arm C.
Cadegiani, control group retrospectively obtained from untreated patients in the same population.
Carvallo, concern about potential data issues.
Carvallo (B), concern about potential data issues.
Carvallo (C), minimal details of groups provided.
de Jesús Ascencio-Montiel, unadjusted results with alternate outcome adjusted results showing significant changes with adjustments. Excluded results: death, mechanical ventilation, hospitalization, progression.
de la Rocha, data mismatch, no response from authors.
Elavarasi, unadjusted results with no group details.
Ferreira, unadjusted results with no group details; substantial unadjusted confounding by indication likely.
Hashmi, baseline severity favors control, post-hoc outcome and SAP changes, see discussion.
Hazan (B), study uses a synthetic control arm.
Hellwig, not a typical trial, analysis of African countries that used or did not use ivermectin prophylaxis for parasitic infections.
IVERCOR PREP, minimal details provided.
Kishoria, excessive unadjusted differences between groups.
López-Medina, strong evidence of patients in the control group self-medicating, ivermectin widely used in the population at that time, and the study drug identity was concealed by using the name D11AX22.
Mikamo, very low risk group with almost no progression leaves little room for improvement, unbalanced baseline dyspnea and high symptom scores, design and post-hoc changes favor null result.
Mustafa, unadjusted results with no group details.
Qadeer, minimal baseline details provided.
Ravikirti, exclusion of patients in less severe condition, data/analysis concerns.
Reis, multiple anomalies as per detailed analysis.
Rezai, multiple critical issues, see study page.
Rezai (B), multiple critical issues, see study page.
Roy, no serious outcomes reported and fast recovery in treatment and control groups, there is little room for a treatment to improve results.
Samajdar, minimal details provided; unadjusted results with no group details; results may be significantly affected by survey bias.
Schilling, post-hoc change to exclude patients treated before high viral load, population very low risk, recovering quickly without treatment, high baseline immunity, 2.2x greater baseline antibody negative for the treatment arm.
Siripongboonsitti, data consistency issues, very low risk patients/variants with almost no progression, all patients received known effective antiviral, baseline differences.
Soto, substantial unadjusted confounding by indication likely; substantial confounding by time possible due to significant changes in SOC and treatment propensity near the start of the pandemic.
Soto-Becerra, substantial unadjusted confounding by indication likely; includes PCR+ patients that may be asymptomatic for COVID-19 but in hospital for other reasons.
Szente Fonseca, result is likely affected by collinearity across treatments in the model.
Tanioka, not a typical trial, analysis of African countries that used or did not use ivermectin prophylaxis for parasitic infections.
Thairu, significant confounding by time possible due to separation of groups in different time periods.
Zubair, substantial unadjusted confounding by indication likely; unadjusted results with no group details.
Figure 20. Random effects meta-analysis
excluding studies with significant issues. Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Heterogeneity in COVID-19 studies arises from many factors including:
The time between infection or the onset of symptoms and
treatment may critically affect how well a treatment works. For example an
antiviral may be very effective when used early but may not be effective in
late stage disease, and may even be harmful. Oseltamivir, for example, is
generally only considered effective for influenza when used within 0-36 or
0-48 hours190,191. Baloxavir marboxil studies for influenza
also show that treatment delay is critical — Ikematsu et al. report
an 86% reduction in cases for post-exposure prophylaxis, Hayden et al.
show a 33 hour reduction in the time to alleviation of symptoms for treatment
within 24 hours and a reduction of 13 hours for treatment within 24-48 hours,
and Kumar et al. report only 2.5 hours improvement for inpatient
treatment.
| Treatment delay | Result |
| Post-exposure prophylaxis | 86% fewer cases192 |
| <24 hours | -33 hours symptoms193 |
| 24-48 hours | -13 hours symptoms193 |
| Inpatients | -2.5 hours to improvement194 |
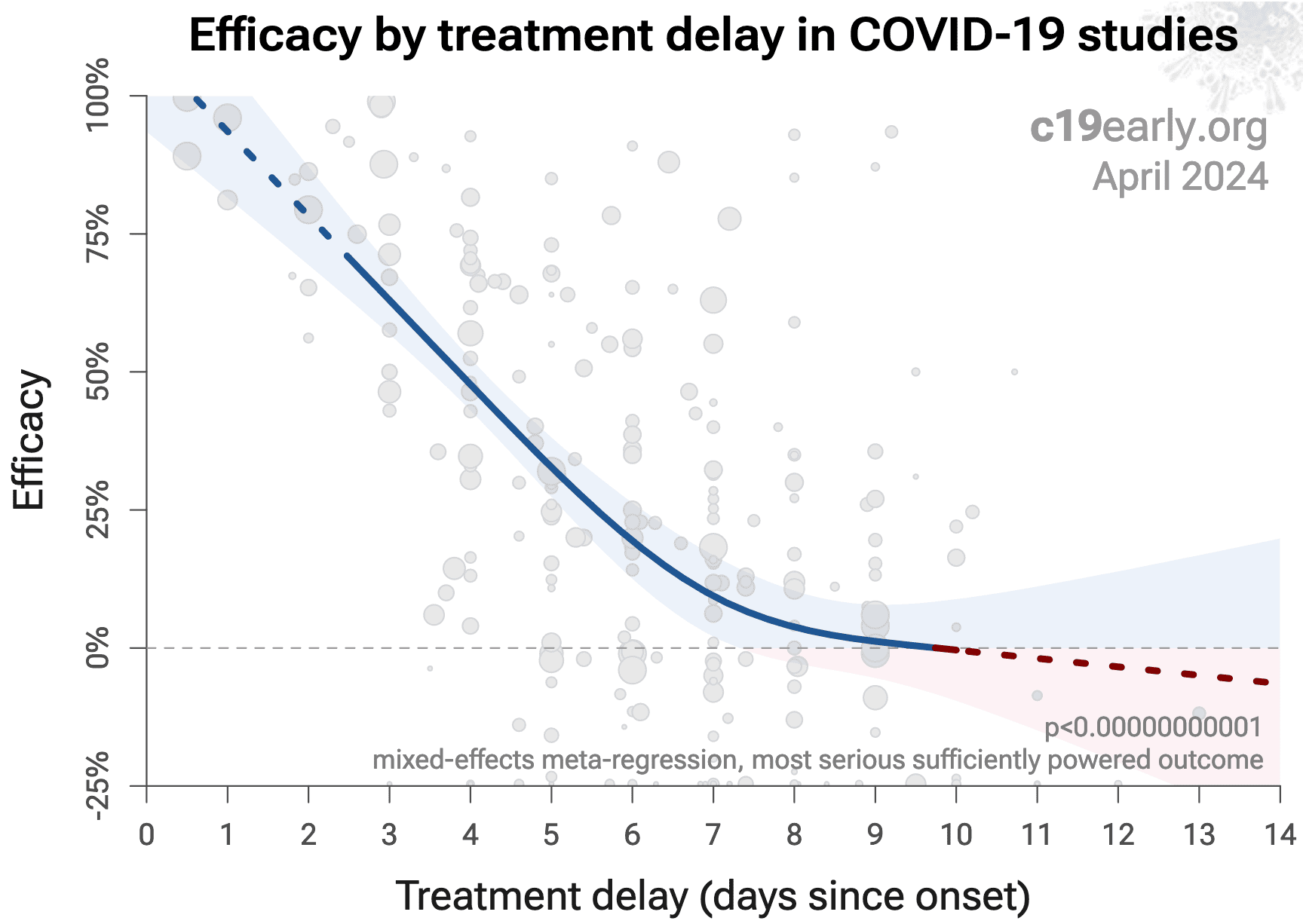
Figure 21 shows a mixed-effects meta-regression for efficacy
as a function of treatment delay in COVID-19 studies from 172 treatments, showing
that efficacy declines rapidly with treatment delay. Early treatment is
critical for COVID-19.
Figure 21. Early treatment is more effective. Meta-regression showing efficacy as a function of treatment delay in COVID-19 studies from 172 treatments.
Details of the patient population including age and comorbidities may
critically affect how well a treatment works. For example, many COVID-19
studies with relatively young low-comorbidity patients show all patients
recovering quickly with or without treatment. In such cases, there is little
room for an effective treatment to improve results, for example as in
López-Medina et al.
Efficacy may depend critically on the distribution of
SARS-CoV-2 variants encountered by patients. Risk varies significantly across
variants195, for example the Gamma variant shows significantly
different characteristics196-199. Different
mechanisms of action may be more or less effective depending on variants, for
example the degree to which TMPRSS2 contributes to viral entry can differ
across variants200,201.
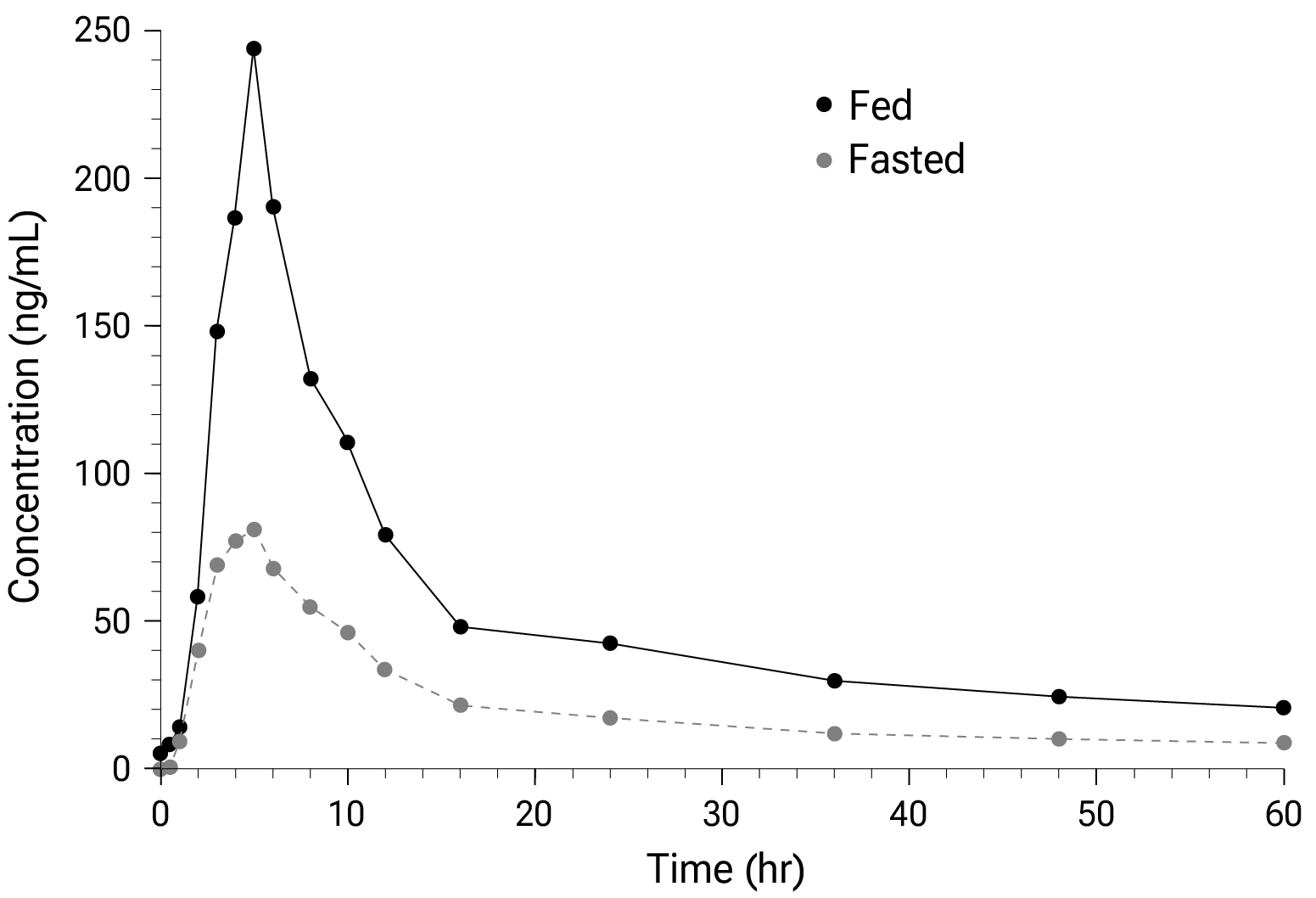
Effectiveness may depend strongly on the dosage and treatment regimen.
Higher dosages have been found
to be more successful for ivermectin202. Method of administration
may also be critical. Guzzo show that the plasma concentration of
ivermectin is much higher when administered with food (Figure 22:
geometric mean AUC 2.6 times higher). Many ivermectin studies specify fasting,
or they do not specify administration. Fasting administration is expected to
reduce effectiveness for COVID-19 due to lower plasma and tissue
concentrations. Note that this is different to anthelmintic use in the
gastrointestinal tract where fasting is recommended.
Figure 22. Ivermectin plasma concentration is significantly higher when administered with a meal. The graph shows mean plasma concentration profiles following single 30mg oral doses for fed and fasted administration, from Guzzo et al.
The quality of medications may vary significantly between
manufacturers and production batches, which may significantly affect efficacy
and safety. Williams et al. analyze ivermectin from 11 different sources,
showing highly variable antiparasitic efficacy across different manufacturers.
Xu et al. analyze a treatment from two different manufacturers, showing 9
different impurities, with significantly different concentrations for each
manufacturer.
Across all
studies there is a strong association between different outcomes, for example
improved recovery is strongly associated with lower mortality. However,
efficacy may differ depending on the effect measured, for example a treatment
may be more effective against secondary complications and have minimal effect
on viral clearance.
The
distribution of studies will alter the outcome of a meta analysis. Consider a
simplified example where everything is equal except for the treatment delay,
and effectiveness decreases to zero or below with increasing delay. If there
are many studies using very late treatment, the outcome may be negative, even
though early treatment is very effective.
All meta analyses combine heterogeneous studies, varying in population,
variants, and potentially all factors above, and therefore may obscure
efficacy by including studies where treatment is less effective. Generally, we
expect the estimated effect size from meta analysis to be less than that for
the optimal case.
Looking at all studies is valuable for providing an overview of all research,
important to avoid cherry-picking, and informative when a positive result is
found despite combining less-optimal situations. However, the resulting
estimate does not apply to specific cases such as
early treatment in high-risk populations.
While we present results for all studies, we also present treatment time and
individual outcome analyses, which may be more informative for specific use
cases.
Ivermectin studies vary widely in all the factors above, which makes the
consistently positive results remarkable. A failure to detect an association
after combining heterogeneous studies does not mean the treatment is not
effective (it may only work in certain cases), however the reverse is not true
— an identified association is valid, although the magnitude of the
effect may be larger for more optimal cases, and lower for less optimal cases.
Note that trial with a design favoring null results have become common, and
are likely to dominate future trials. For example, the Together Trial tested
ivermectin in locations known to have a high degree of self-medication, up to
7 days from onset (while claiming to be an early treatment trial), and using
low doses compared to clinical recommendations for the dominant variant. The
ACTIV-6 trial had a median treatment delay of 6 days and very low risk
patients.
This section validates the use of pooled effects for COVID-19, which enables
earlier detection of efficacy, however pooled effects are no longer required
for ivermectin as of September 2020. Efficacy is now known based on specific outcomes for all studies and when restricted to RCTs. Efficacy based on specific outcomes was delayed by 1.3 months compared to using pooled outcomes.
For COVID-19, delay in clinical results translates into
additional death and morbidity, as well as additional economic and societal
damage. Combining the results of studies reporting different outcomes is
required.
There may be no mortality in a trial with low-risk patients,
however a reduction in severity or improved viral clearance may translate
into lower mortality in a high-risk population.
Different studies may report lower severity, improved recovery, and lower mortality,
and the significance may be very high when combining the results.
"The studies reported different outcomes" is not a good reason for
disregarding results.
Pooling the results of studies reporting different outcomes allows us to use
more of the available information. Logically we should, and do, use additional
information when evaluating treatments—for example dose-response and
treatment delay-response relationships provide additional evidence of efficacy
that is considered when reviewing the evidence for a treatment.
We present both specific outcome and pooled analyses.
In order to combine the results of studies reporting different outcomes we use
the most serious outcome reported in each study, based on the thesis that
improvement in the most serious outcome provides comparable measures of
efficacy for a treatment. A critical advantage of this approach is
simplicity and transparency.
There are many other ways to combine evidence for different outcomes, along
with additional evidence such as dose-response relationships, however these
increase complexity.
Trials with high-risk patients may be restricted due to ethics for treatments
that are known or expected to be effective, and they increase difficulty for
recruiting. Using less severe outcomes as a proxy for more serious outcomes
allows faster and safer collection of evidence.
For many COVID-19 treatments, a reduction in mortality logically
follows from a reduction in hospitalization, which follows from a reduction in
symptomatic cases, which follows from a reduction in PCR positivity. We can
directly test this for COVID-19.
Analysis of the the association between different outcomes across studies from
all 172
treatments we cover confirms the validity of pooled outcome analysis for COVID-19.
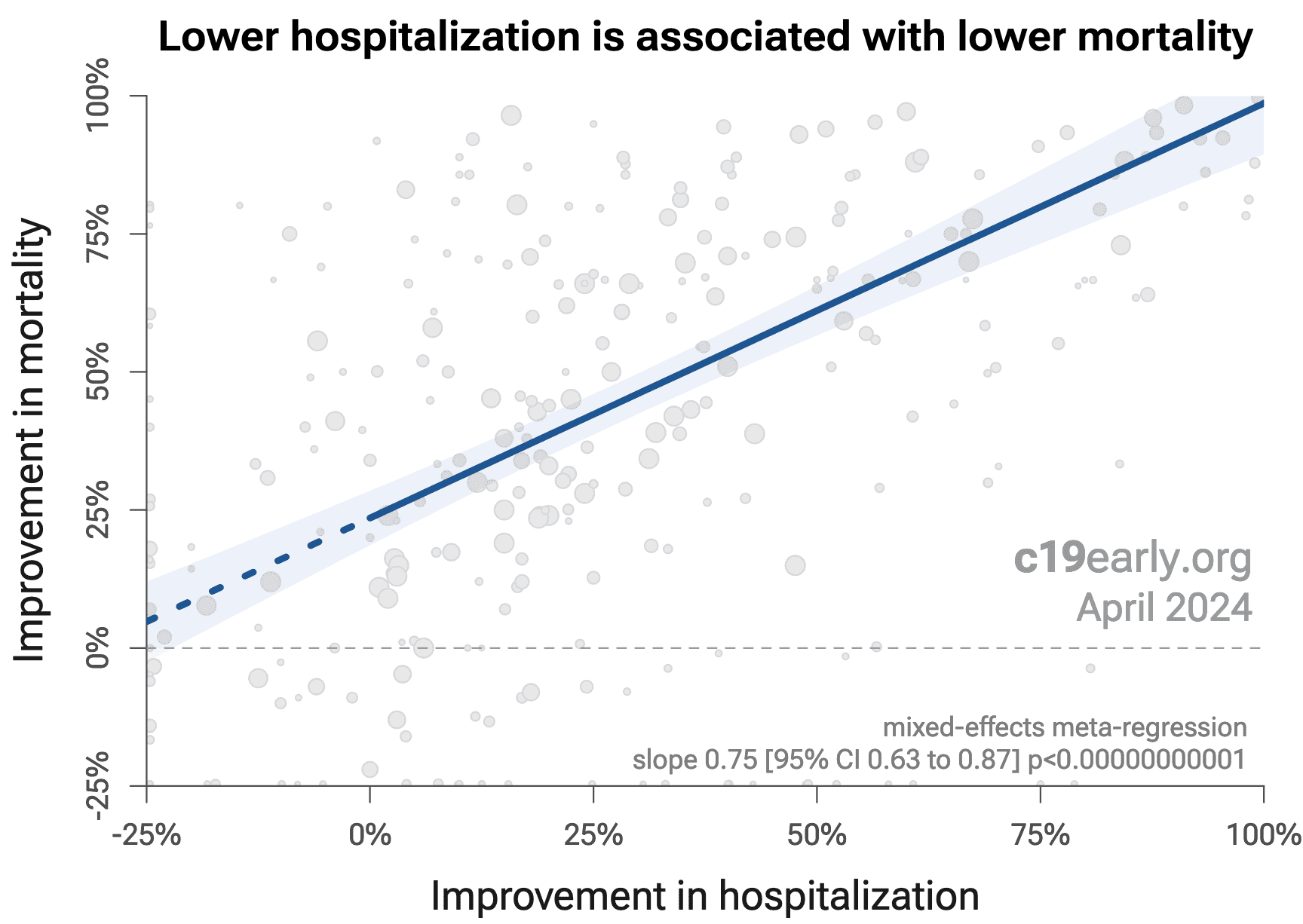
Figure 23 shows that lower hospitalization is very strongly associated
with lower mortality (p < 0.000000000001).
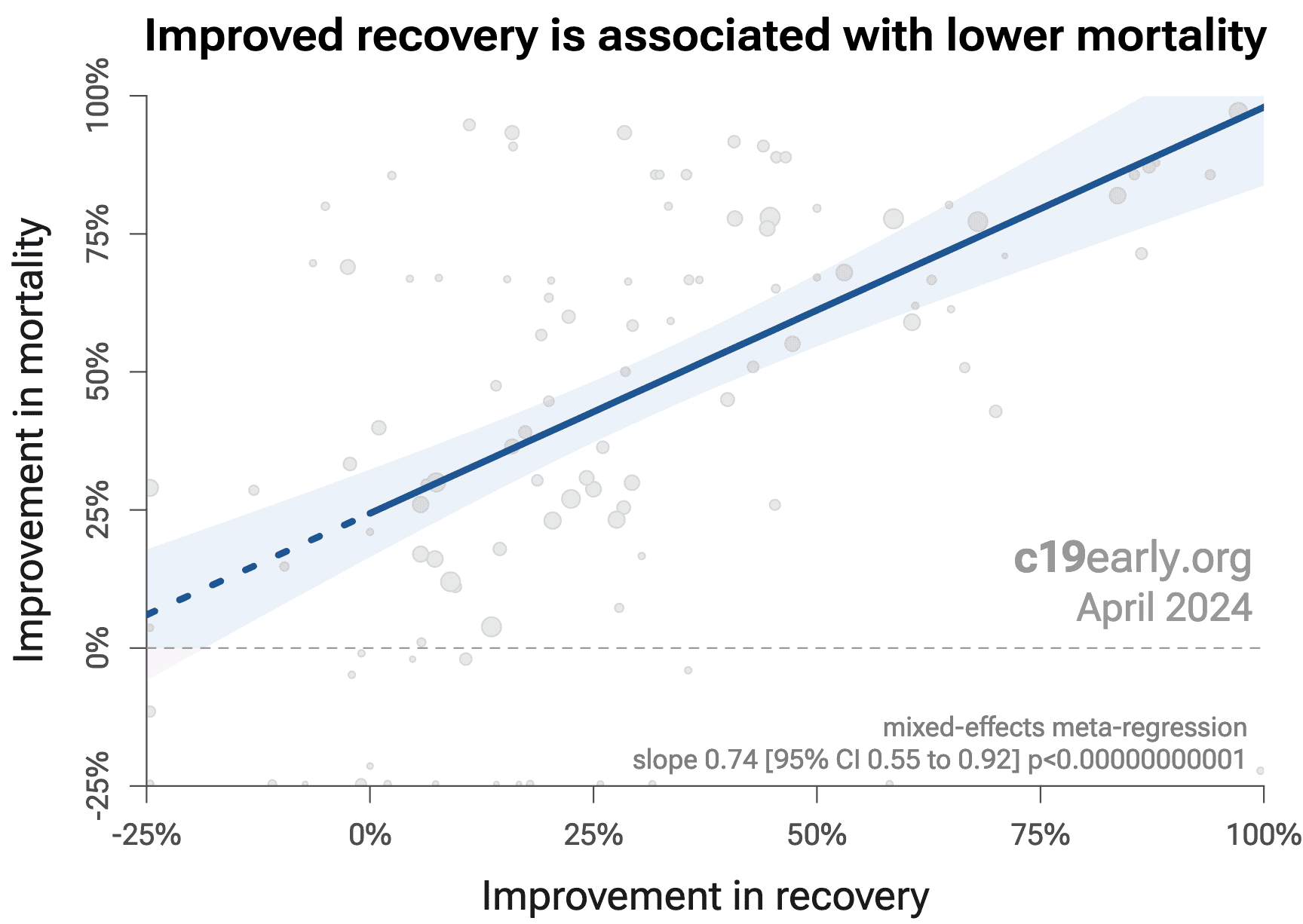
Similarly, Figure 24 shows that improved recovery is very strongly associated
with lower mortality (p < 0.000000000001).
Considering the extremes, Singh et al. show an association between viral clearance and
hospitalization or death, with p = 0.003 after excluding one large
outlier from a mutagenic treatment, and based on 44 RCTs including 52,384
patients.
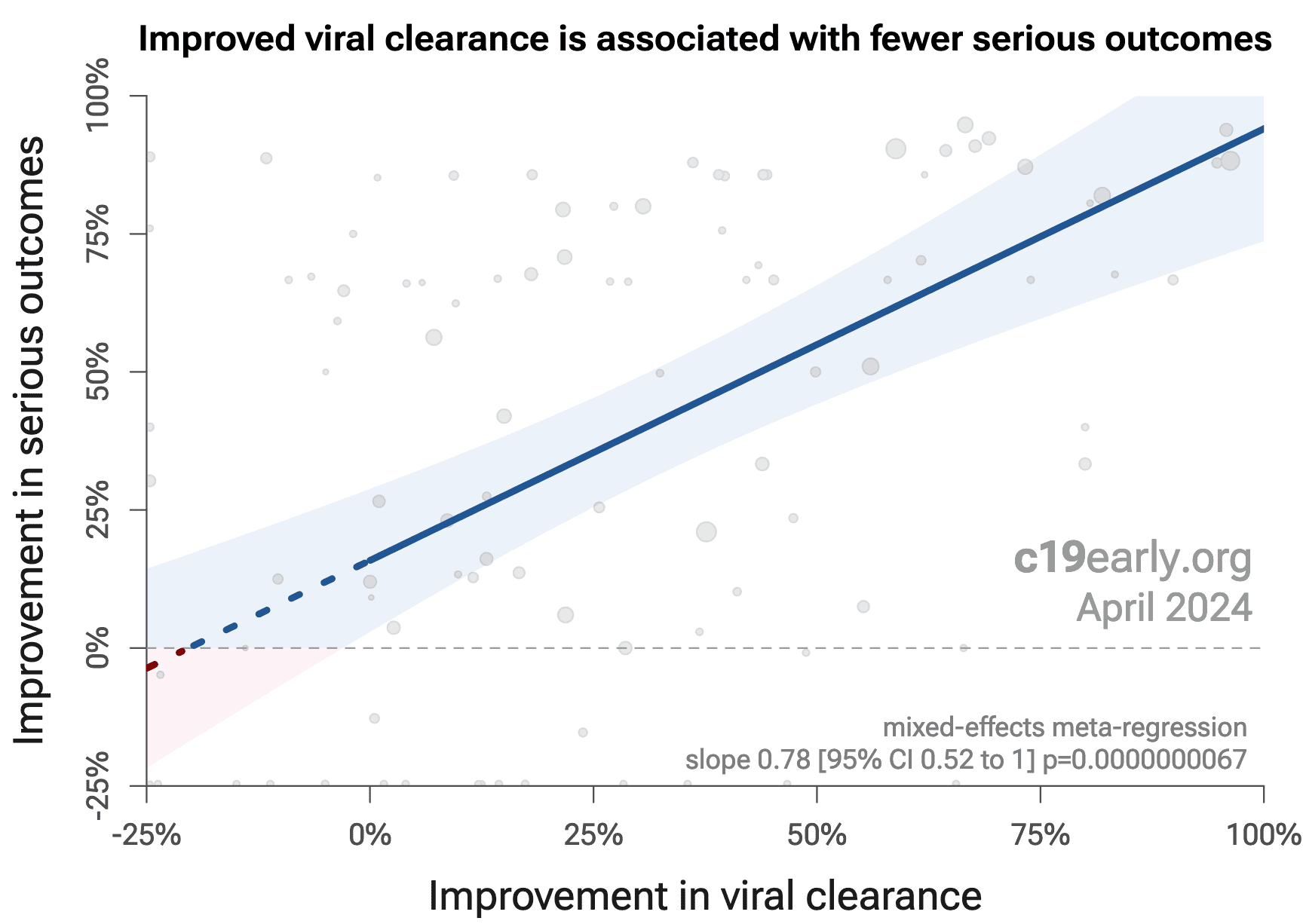
Figure 25 shows that improved viral clearance is strongly associated
with fewer serious outcomes. The association is very similar to
Singh et al., with higher confidence due to the larger number of
studies. As with Singh et al., the confidence increases
when excluding the outlier treatment, from p = 0.000000082 to p = 0.0000000033.
Figure 23. Lower hospitalization is associated with lower mortality, supporting pooled outcome analysis.
Figure 24. Improved recovery is associated with lower mortality, supporting pooled outcome analysis.
Figure 23. Improved viral clearance is associated with fewer serious outcomes, supporting pooled outcome analysis.
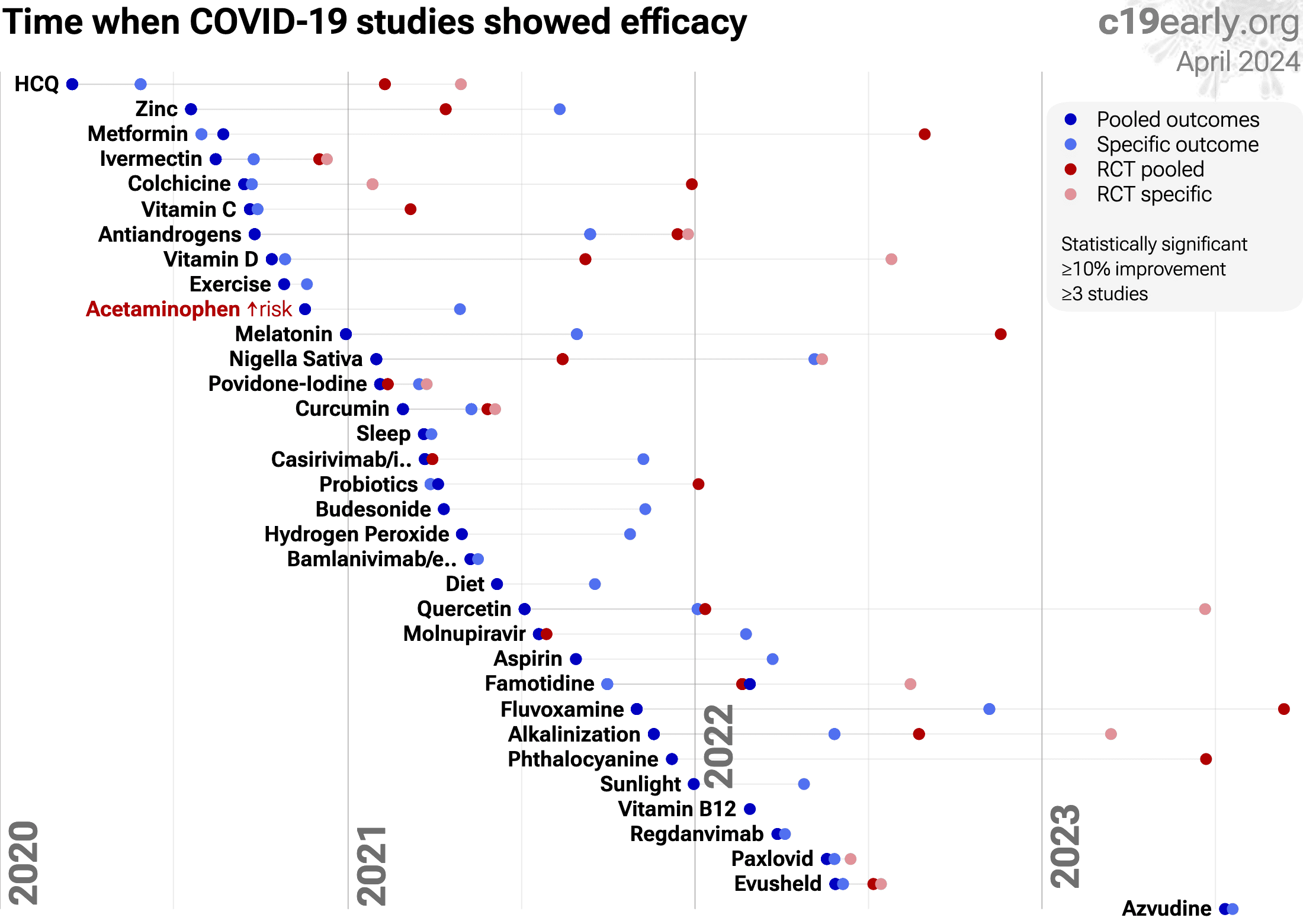
Currently, 55 of the treatments we analyze show statistically significant efficacy or harm, defined as ≥10% decreased risk or >0% increased risk from ≥3 studies. 88% of these have been confirmed with one or more specific outcomes, with a mean delay of 4.9 months. When restricting to RCTs only, 57% of treatments showing statistically significant efficacy/harm with pooled effects have been confirmed with one or more specific outcomes, with a mean delay of 7.3 months.
Figure 26 shows when treatments were found effective during the
pandemic. Pooled outcomes often resulted in earlier detection of efficacy.
Figure 26. The time when studies showed that
treatments were effective, defined as statistically significant improvement of
≥10% from ≥3 studies.
Pooled results typically show efficacy earlier than specific
outcome results. Results from all studies often shows efficacy much earlier
than when restricting to RCTs.
Results reflect conditions as used in trials to date, these depend on the
population treated, treatment delay, and treatment regimen.
Pooled analysis could hide efficacy, for example a treatment that is
beneficial for late stage patients but has no effect on viral clearance may
show no efficacy if most studies only examine viral clearance. In practice, it
is rare for a non-antiviral treatment to report viral clearance and to not
report clinical outcomes; and in practice other sources of heterogeneity such
as difference in treatment delay is more likely to hide efficacy.
Analysis validates the use of pooled effects and shows significantly faster
detection of efficacy on average.
However, as with all meta analyses, it is important to review the different
studies included. We also present individual outcome analyses, which may be
more informative for specific use cases.
WHO updated their treatment recommendations on 3/30/2021217. For ivermectin they reported a mortality odds ratio of
0.19 [0.09-0.36] based on 7 studies with 1,419 patients. They do not specify
which trials they included. The report is inconsistent, with a forest plot
that only shows 4 studies with mortality results. WHO's recommendation has not
been updated for days.
Despite this extremely positive result, they recommended only
using ivermectin in clinical trials. The analysis contains many flaws218:
•Of the
105 studies (52 RCTs), they only
included 16.
•They excluded all
17 prophylaxis studies
(4 RCTs).
•There was no protocol for data
exclusion.
•Trials included in the original
UNITAID search protocol were excluded.
•They excluded all epidemiological
evidence, although WHO has considered such evidence in the past.
•They combine early treatment and late
treatment studies and do not provide heterogeneity information. As above,
early treatment is more successful, so pooling late treatment studies will
obscure the effectiveness of early treatment. They chose not to do subgroup
analysis by disease severity across trials, although treatment delay is
clearly a critical factor in COVID-19 treatment, the analysis is easily done
(as above), and it is well known that the studies for ivermectin and many
other treatments clearly show greater effectiveness for early treatment.
•WHO downgraded the quality of trials
compared to the UNITAID systematic review team and a separate
international expert guideline group that has long worked with the WHO5.
•They disregarded their own guidelines
that stipulate quality assessments should be upgraded when there is evidence
of a large magnitude effect (which there is), and when there is evidence of a
dose-response relationship (which there is). They claim there is no
dose-response relationship, while the UNITAID systematic review team found a
clear relationship, along with individual studies202.
•Their risk of bias assessments do not
match the actual risk of bias in studies. For example they classify
López-Medina as low risk of bias, however this study has many issues
making the results unreliable219, even prompting an open
letter from over 170 physicians concluding that the study is fatally flawed220. Beltran Gonzalez is also classified as low risk
of bias, but is a study with very late stage severe condition high-comorbidity
patients. There is a clear treatment delay-response relationship and very late
stage treatment is not expected to be as effective as early treatment.
Conversely, much higher quality studies were classified as high risk of
bias.
•Although WHO's analysis is called a
"living guideline", it is rarely updated and very out of date. As of May 14,
2021, four of the missing RCTs are known to WHO and labeled "RCTs pending data
extraction"221. We added these 4, 4, 2, and one month
earlier.
•A single person served as Methods
Chair, member of the Guidance Support Collaboraton Committee, and member of
the Living Systematic Review/NMA team.
•Public statements from people involved
in the analysis suggest substantial bias. For example, a co-chair reportedly
said that "the data available was sparse and likely based on chance"222. The clinical team lead refers to their analysis of
ivermectin as "fighting this overuse of unproven therapies ... without
evidence of efficacy"222, despite the extensive evidence of
efficacy from the 105 studies by
1,206 scientists with
220,423 patients. People involved may be
more favorable to late stage treatment of COVID-19, for example the co-chair
recommended treating severe COVID-19 with remdesivir223.
In summary, although WHO's analysis predicts that over 2
million fewer people would be dead if ivermectin was used from early in the
pandemic, they recommend against use outside trials. This appears to be based
primarily on excluding the majority of the evidence, and by assigning bias
estimates that do not match the actual risk of bias in studies.
Use early in the pandemic was proposed by Kitasato University
including the co-discoverer of ivermectin, Dr. Satoshi Ōmura. They requested
Merck conduct clinical trials of ivermectin for COVID-19 in Japan, because
Merck has priority to submit an application for an expansion of ivermectinʼs
indications. Merck declined224.
Merck has recommended against ivermectin225, however this recommendation has not been updated for days.
They stated that there is "no scientific basis for a
potential therapeutic effect against COVID-19 from pre-clinical studies".
This is contradicted numerous studies, including Jitobaom, Li, Fauquet, Boschi, Shahin, Abd-Elmawla, Ma, Vottero, Mody, Parvez, Gao, Bagheri-Far, Zhang, DiNicolantonio, Zhao, Liu (B), Liu (C), Gayozo, Kofler, Munson, Yan, Lefebvre, Haque, de Oliveira Só, Agamah, Oranu, Chellasamy, Umar, Alvarado, Aminpour, Parvez (B), Francés-Monerris, González-Paz, González-Paz (B), Rana, Muthusamy, Qureshi, Schöning, Bello, Udofia, Choudhury, Kern, Saha (B), Eweas, Francés-Monerris (B), Kalhor, Swargiary, Maurya, Lehrer, Suravajhala, García-Aguilar, De Forni, Saha (C), Jitobaom (B), Croci, Zheng, Delandre, Segatori, Jitobaom (C), Mountain Valley MD, Yesilbag, Jeffreys, Surnar, Caly, Uematsu, Albariqi, Errecalde, Madrid, de Melo, Arévalo, Chaccour, Zatloukal, Zaidi, Wehbe, Kalfas, Jans, Heidary .
They state that there is "no meaningful evidence for
clinical activity or clinical efficacy in patients with COVID-19 disease".
This is contradicted by numerous studies including
de Jesús Ascencio-Montiel, Babalola, Chowdhury, Espitia-Hernandez, Mahmud, Chaccour (B), Ghauri, Ravikirti (B), Bukhari, Mohan, Elalfy, Chahla, Mourya, Loue, Merino, Faisal, Aref, Mayer, Manomaipiboon, Khan, Hashim, Budhiraja, Okumuş, Lima-Morales, Huvemek, Baguma, Shimizu, Aref (B), Varnaseri, Behera, Bernigaud, Alam, Chahla (B), Behera (B), Seet, Morgenstern, Mondal, Kerr .
They also claim that there is "a concerning lack of safety
data in the majority of studies". Safety analysis is found in
Guzzo, Kory, Descotes, Errecalde, Madrid , and safety data can be found
in most studies, including
López-Medina, Vallejos, Shahbaznejad, Kishoria, Carvallo (C), Hazan (B), Szente Fonseca, Zubair, Babalola, Chowdhury, Espitia-Hernandez, Mahmud, Chaccour (B), Ghauri, Bukhari, Mohan, Elalfy, Mourya, Loue, Aref, Khan, Okumuş, Lima-Morales, Huvemek, Chahla (B), Behera (B), Seet, Morgenstern, Ahmed, Biber, Krolewiecki, Gorial, Camprubí, Spoorthi, Pott-Junior, Abd-Elsalam, George, Shouman (B), Bhattacharya .
Merck has a number of conflicts of interest:
•Merck has committed to give ivermectin
away for free "as much as needed, for as long as needed" in the
Mectizan® Donation Program279, to help eliminate river
blindness.
•Merck has their own new COVID-19
treatments MK-7110 (formerly CD24Fc)280 and Molnupiravir
(MK-4482)281,282. Merck has a ~$US1.2B agreement
to supply molnupiravir to the US government, if it receives EUA or approval283. Over $US10B in near-term orders are expected if
approved284.
•Ivermectin is off-patent, there are
many manufacturers, and Merck is unlikely to be able to compete with low cost
manufacturers.
•Promoting the use of low cost
off-patent medications compared to new products may be undesirable to some
shareholders.
•Japan requested Merck conduct clinical
trials early in the pandemic and they declined. Merck may be reluctant to
admit this mistake224.
For other concerns regarding Merck's statement and prior
actions related to Vioxx, see Scheim (D).
The US FDA recommended against ivermectin on March 5, 2021,
however they stated that "The FDA has not reviewed data to support use of
ivermectin in COVID-19 patients to treat or to prevent COVID-19". There
is still no indication that the FDA has reviewed the clinical trials days later.
The FDA notes that they "received multiple reports of
patients who have required medical support and been hospitalized after
self-medicating with ivermectin intended for horses". The number of
reports was 4286. For comparison, acetaminophen overdose
results in ~33,000 yearly hospitalizations in the USA (~12,000 unintentional)287. The FDA's recommendation may increase cases of
self-medication with animal ivermectin, because it reduces the percentage of
prescribing physicians.
They state that "Ivermectin is not an anti-viral", however
many studies contradict this Caly, Buonfrate, Qadeer, Thairu, Babalola, Chowdhury, Espitia-Hernandez, Mahmud, Bukhari, Mohan, Elalfy, Mourya, Aref, Khan, Okumuş, Ahmed, Biber, Wijewickrema, Rezk , including 11 RCTs.
They note that "some initial research is underway",
however there had been many studies completed and published prior to the FDA
recommendation: López-Medina, Beltran Gonzalez, Hellwig, Cadegiani, Carvallo (C), Babalola, Chowdhury, Espitia-Hernandez, Mahmud, Chaccour (B), Ghauri, Ravikirti (B), Bukhari, Mohan, Elalfy, Khan, Hashim, Budhiraja, Okumuş, Lima-Morales, Behera, Bernigaud, Alam, Chahla (B), Ahmed, Biber, Gorial, Camprubí, Spoorthi, Shouman (B), Podder, Chachar, Rajter , including 17 RCTs.
Sep 3, 2021: The FDA revised their statement slightly.
They removed the false claim that invermectin is not an antiviral, and they
removed the statement that they have not reviewed the data. However, there is
still nothing to indicate that they have reviewed the clinical trials.
Indeed, they state "currently available data do not show ivermectin is
effective against COVID-19" and "ivermectin has not been shown to be safe or
effective for these indications", which are both false.
Update: NIH has updated the recommendation, based heavily on
the Together Trial, while making no mention of the impossible data, blinding, randomization, and protocol
failures, or that the co-principal investigator privately reported that "There is a clear signal that IVM works in COVID
patients".
NIH has reported that there is insufficient evidence to
recommended for or against ivermectin293.
A table with summaries of 7 studies is provided, dated Dec 16, 2021, and they
reference another 23 studies without analysis, however there are
105 studies to date. No quantitative analysis is
provided. The NIH recommendation is "insufficient evidence", indicating that
they must review new evidence immediately. Lack of updates suggest bias.
The likely members of the panel have been revealed by FOIA
requests294. In the first request, all but two member names were
redacted295,
however all are visible in a second request296.
Major conflicts of interest have been reported294,297.
7 of 9 panel members appear to have conflicts of interest. Submit Corrections or Updates
| Prof. Adaora Adimora | |
| Prof. Roger Bedimo | |
| Prof. Rajesh Gandhi |
•Gilead: grants, advisory board, personal fees304,305
"Dr. Gandhi reports grants and personal fees from Gilead, personal fees from Merck, grants and personal fees from Theratechnologies, grants from ViiV, grants from Janssen."
•Janssen: grants304
•Open Payments shows $45,000 from Merck and
$10,000 from Gilead306
|
| Prof. David Glidden | |
| Prof. Roy Gulick |
•Merck: grants307
(deleted from current version308)
"Roy M. Gulick, MD, MPH, has disclosed that he has received grants for
clinical research from Abbott, Boehringer Ingelheim, Merck, Pfizer, Schering,
and Tibotec, and has received grants for educational activities from Gilead
and Monogram. Dr. Gulick has also disclosed that he has served as an ad-hoc
advisor or consultant to Abbott, Boehringer Ingelheim, Bristol-Myers Squibb,
Gilead, GlaxoSmithKline, Pfizer, Schering, and Tibotec", principal investigator
on A5391 with funding in part from Merck309
|
| Prof. Susanna Naggie | |
| Prof. Andrew Pavia |
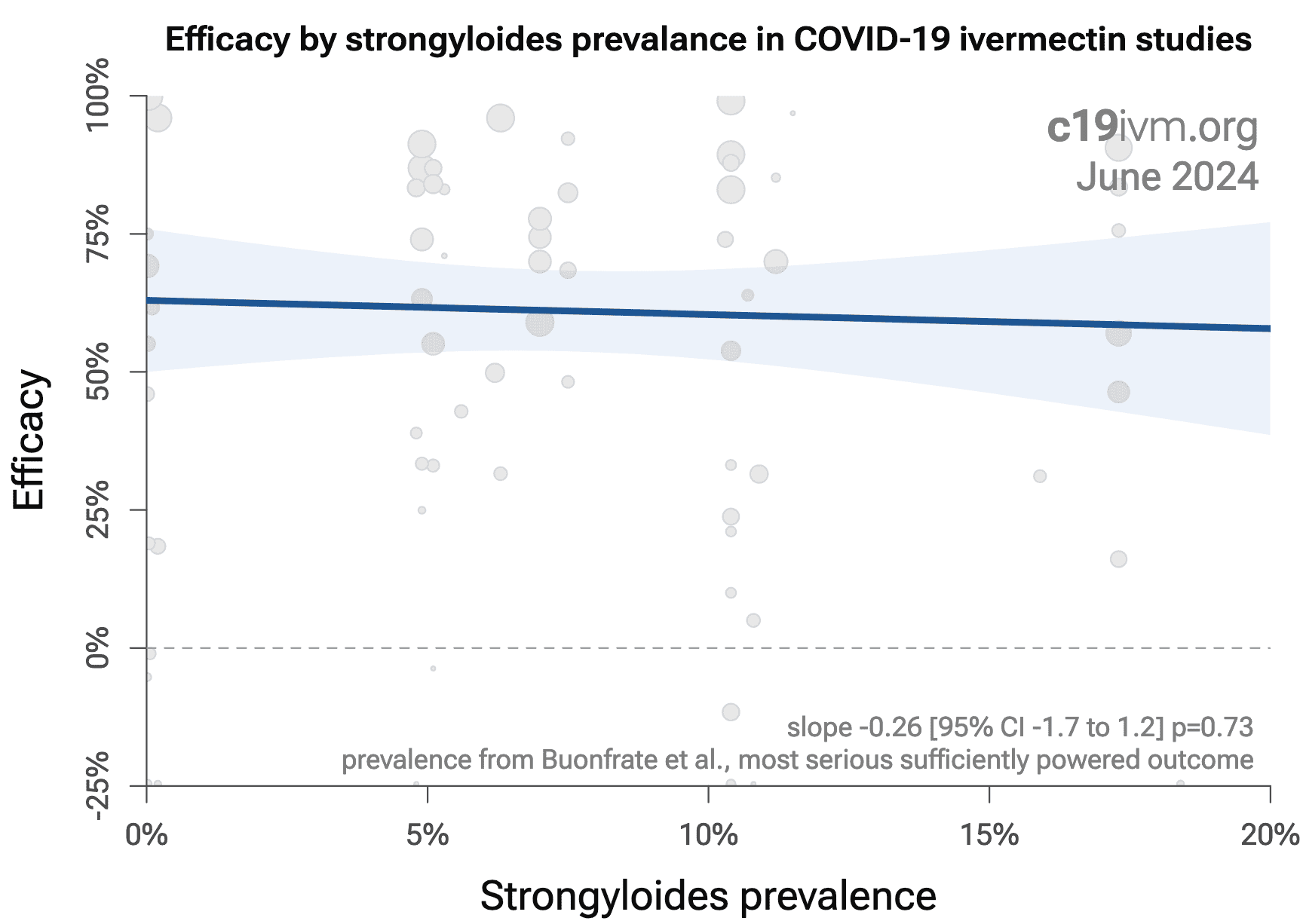
One theory for the beneficial effect of ivermectin for COVID-19
is related to strongyloides and the use of steroids — control group
patients with strongyloides may be at risk due to steroid use, while
ivermectin patients are protected. While this mechanism may contribute to
efficacy in some cases, it is inconsistent with the data. If this was the
case, we would expect to see greater benefit in late stage trials where
steroids are used more often, and we would expect to see greater benefit for
outcomes that occur after steroids are used. However, we see a very strong
opposite effect for treatment time, and we see comparable or stronger efficacy
for earlier outcomes.
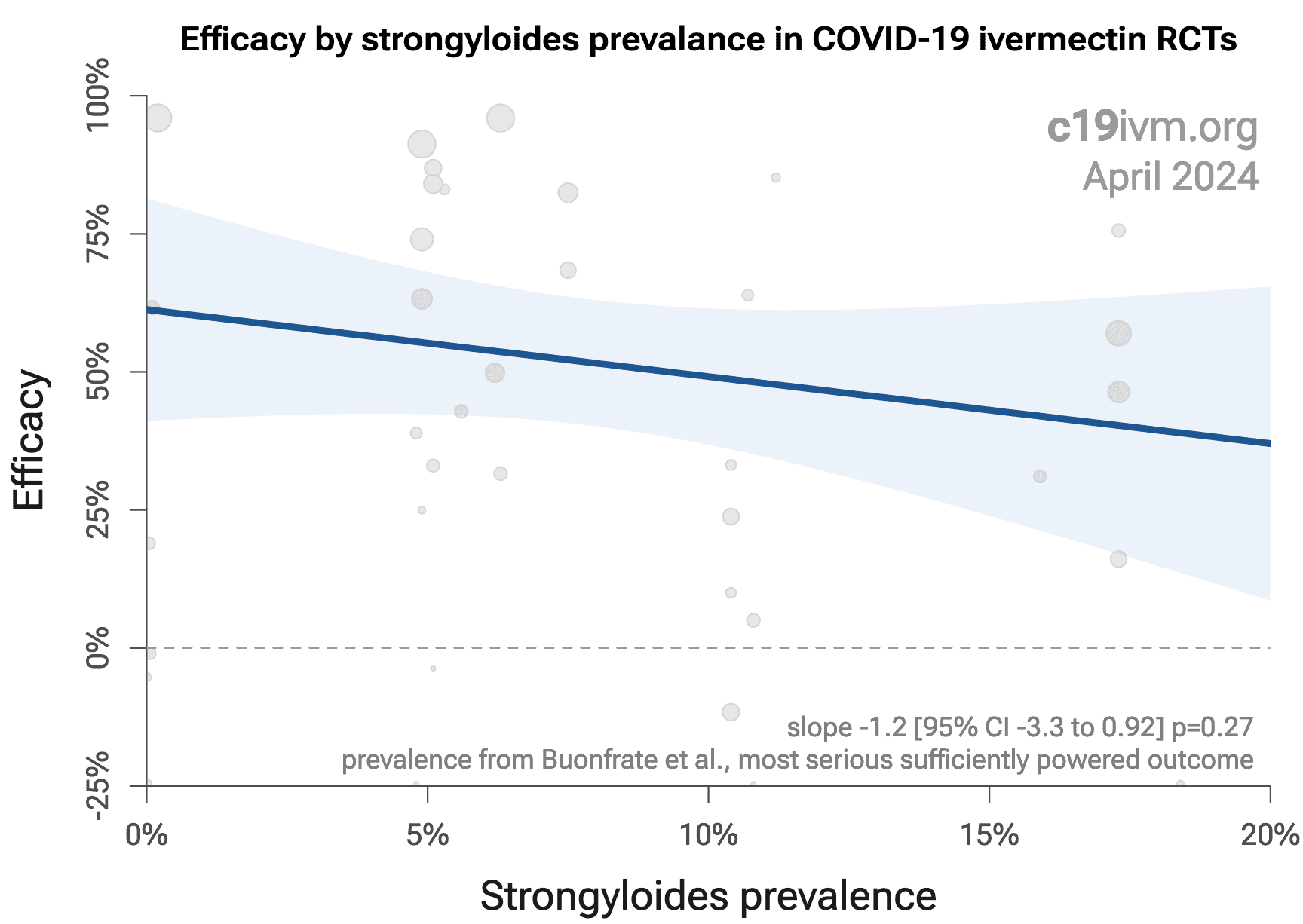
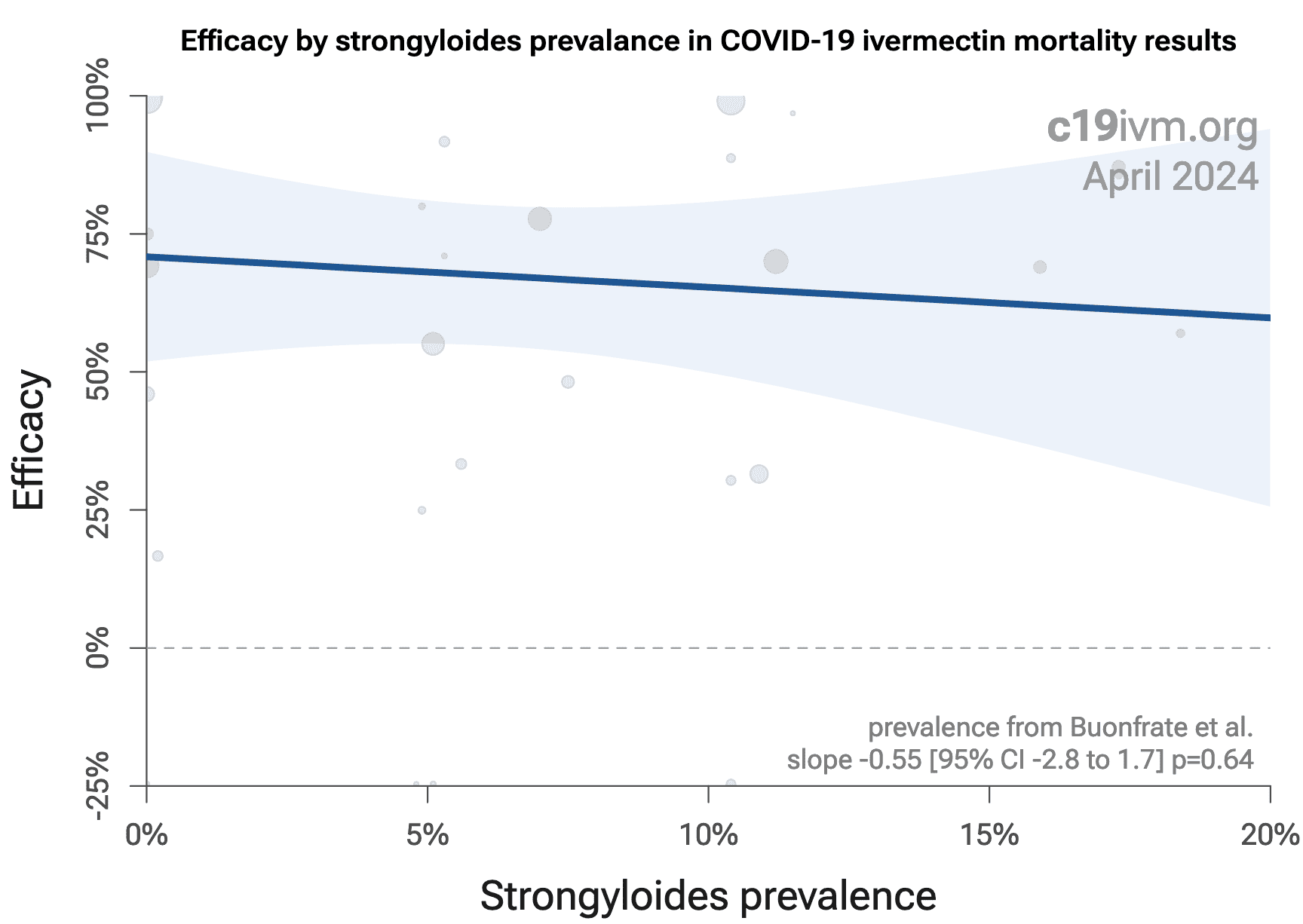
The theory has gained renewed interest based on a new analysis
by Bitterman et al.. However, this analysis is confounded by treatment
delay, dose, conflicts of interest, and other factors, and the effect
disappears when analyzing all studies, all RCTs, or all mortality results, as
shown in Figure 27.
Although the first author has responded to the confounders on
Twitter, we do not see mention of them in the paper. Author is also aware that
the larger sets of all trials, all RCTs, or all mortality results do not show
the effect, however we also do not see this mentioned in the paper. These
omissions suggest investigator bias. Author claims they could not discuss
these issues due to publication delays, however the paper was accepted Jan 31,
2022, and author was aware of the issues months before, for example discussing
treatment delay and dose in Nov 2021. These confounders are also basic and not
really possible to miss.
The meta analysis for Hashim includes critical
patients, however these patients were always allocated to the treatment arm
for ethical reasons, therefore including them is not logical and introduces
substantial bias. According to the author response, this appears to have been
known, suggesting investigator bias. Authors include Shahbaznejad
where the only death was a critical patient that died within 24 hours of
admission.
Although authors note following PRISMA guidelines, we do not
see registration of the protocol or discussion thereof. We note that the
current protocol is the result of multiple changes to the original methodology
as posted on Twitter: from 3 groups to 2 groups, altering the included
studies, and switching from using one source for prevalence estimates to
selecting estimate sources on a per study basis, which allows potential bias
in the selection. Notably, this resulted in moving the Together Trial (Brazil)
into the low prevalence category.
Author's results rely on trials with a very small number of
mortality events — the high stronglyoides prevalance group has trials
with 1, 3, 4, and 13 events. Authors do mention limitations due to the small
number of events and the reliability of strongyloides estimates.
Authors indicate no conflicts of interest, however the first
author has been an investigator on a Pfizer trial, which may be NCT04092452, showing
completion in January 2022315,316.
Figure 27. Mixed-effects meta-regression showing efficacy as a function of strongyloides prevalence. A. all studies. B. all RCTs. C. all mortality results.
The following refers to the first author's analysis posted
earlier on Twitter. The author selected 10 of the
105 studies, with 3 in a high strongyloides
prevalence group where a greater benefit is seen. This was used to draw strong
conclusions about the mechanism of ivermectin efficacy.
There are several limitations to this analysis. One of the 3
studies does not mention steroids in the list of SOC medications, while a
second reports 6% usage for the control group. Author has added a fourth paper
in a revised grouping with 11 studies.
We perfomed a similar analysis for all studies (except the 2
ecological studies), which shows no significant effect, with the high
prevalence group actually showing lower improvement (49% [34‑61%] vs. 65% [57‑71%] for the low prevalence
group). Details can be found in the
supplementary data. Results are similar
when restricting to mortality results or when restricting to RCTs.
Why does the smaller analysis with 11 studies show a greater
benefit in high strongyloides prevalence regions? The effect is based on
relatively few events - 1, 3, 4, and 13 respectively for the high prevalence
group. More importantly, the result is confounded by treatment delay and
dose.
Treatment delay. All meta analyses combine heterogeneous
studies which results in limitations. For example in pooled analysis we
combine hospitalization and mortality. In terms of evaluating efficacy for
COVID-19 treatments, reduction in hospitalization reasonably leads to
reduction in mortality for high-risk populations. Both are indicators of
efficacy, and both are valuable. In the largest series of COVID-19 treatment
trials, hospitalization and mortality estimates are very similar. The same
does not apply to treatment delay for antivirals. A trial showing efficacy
with early treatment provides no information on late treatment, and a trial
showing no efficacy with late treatment provides no information on early
treatment. Ivermectin, as with many COVID-19 treatments, shows a strong
treatment delay relationship — early treatment shows significantly
higher efficacy.
The high prevalence group in the 11 study analysis has more
early treatment trials, and the low prevalence group has more late treatment
trials. The result is confounded by treatment delay, and reflects the greater
efficacy of early treatment.
Only one trial in the high prevalence group is classified as
late treatment, I-TECH, which was very close to the cutoff. Moreover, of all
trials in the 11 trial analysis, this one uses the highest dose.
Dose. The average dosage used in the high prevalence
group is about twice the dose in the low prevalence group, and would be close
to three times higher if the Together Trial was not moved to the low
prevalence group. The result is confounded by dose, and reflects the greater
efficacy of higher dosages.
Variants. Efficacy may vary based on variants. Notably,
the Gamma variant was most common for one trial in the low prevalance group.
This variant shows dramatically different characteristics199,
and clinicians report that significantly higher dosage and/or earlier
treatment is required, as may be expected for variants where the peak viral
load is significantly higher and/or reached earlier196,197.
Conflicts of interest. Two trials have very high
(>$US1B) negative conflicts of interest which may introduce bias towards null
effects. The trial in the low prevalance group shows a lower effect size. The
trial in the high prevalence group also shows a lower effect size for the
primary outcome. This trial shows a larger mortality effect, however with only
one event this has very low significance.
Summary. In summary, the greater benefit in high
strongyloides prevalence regions is only seen with the small subset of 11
trials and is not seen with all trials, or after restriction to mortality
results, or restriction to RCTs. Within the 11 trial sample, all trials except
one in the low prevalence group have confounding due to treatment delay and/or
low dosage, where a lower effect size is expected. The only remaining trial in
the group is unpublished, has an unknown treatment delay (a significant
percentage of patients may have been treated very late), has very high
negative conflicts of interest, and the Gamma variant was most common, in
addition to other issues.
Some authors claim that Caly showed that therapeutic
concentrations are not easily reached in humans. This is incorrect. The authors
explain why their in vitro study cannot be used to determine the
effective dose in vivo, and state that the
concentration required is very unlikely to be an issue317.
The study used monkey
kidney cells (the only choice at the time of the experiments), which
lack adaptive immune responses and do not produce interferon. Authors
also note that ivermectin accumulates in lung and other tissues, that
subsequent experiments with lung cells show many times greater
concentrations, and that the average lung concentration shown in modeling
studies exceeds the effective level shown in their research.
Tissue concentrations of ivermectin can be much higher than plasma
concentration318,319.
Authors note that ivermectin works with the immune system and a 1:1 ratio of
drug to virus is unlikely to be required. In Bray, authors reply
that "ivermectin's key direct target in mammalian cells is a not a viral
component, but a host protein important in intracellular transport; the fact
that it is a host-directed agent (HDA) is almost certainly the basis of its
broad-spectrum activity against a number of different RNA viruses in vitro.
The way a HDA can reduce viral load is by inhibiting a key cellular process
that the virus hijacks to enhance infection by suppressing the host antiviral
response. Reducing viral load by even a modest amount by using a HDA at low
dose early in infection can be the key to enabling the body's immune system to
begin to mount the full antiviral response before the infection takes
control." In further research, authors note that they find efficacy for
prophylactic use, and that smaller repeated doses are more efffective than a
single larger dose317.
Moreover, there are now 26 In Vitro studies that support the
efficacy of ivermectin for COVID-1940,46,49,50,52,56,65,68,69,72,74,78,107-120 .
Publishing is often biased towards positive results, which we
would need to adjust for when analyzing the percentage of positive results.
For ivermectin, there is strong evidence of a growing negative publication
bias.
As Scott Alexander said in November
2021, "if you say anything in favor of ivermectin you will be cast out
of civilization and thrown into the circle of social hell reserved for Klan
members and 1/6 insurrectionists. All the health officials in the world will
shout 'horse dewormer!' at you and compare you to Josef Mengele." In many
locations, publishing positive ivermectin results is not conducive to
maintaining employment or friendships. This can be seen in the design of
recent trials, and the extreme measures taken to avoid presenting
statistically significant positive results, as detailed in the study notes
below.
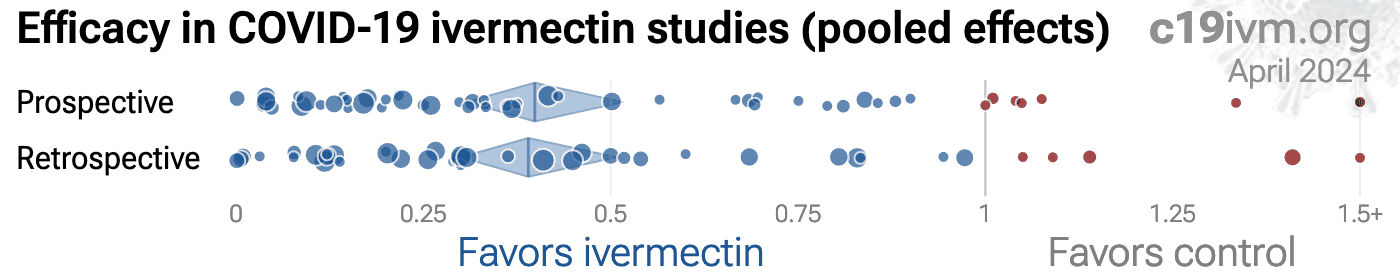
One method to evaluate bias is to compare prospective vs.
retrospective studies, although this method has become less useful with
ivermectin due to the increase of prospective studies with designs favoring
null results. Prospective studies are likely to be published regardless of the
result, while retrospective studies are more likely to exhibit bias. For
example, researchers may perform preliminary analysis with minimal effort and
the results may influence their decision to continue. Retrospective studies
also provide more opportunities for the specifics of data extraction and
adjustments to influence results. Figure 28 shows a scatter plot of
results for prospective and retrospective studies.
Prospective studies show 59% [48‑68%] improvement in meta
analysis, compared to 61% [49‑70%] for retrospective studies,
showing no significant difference.
Bryant also perform a
funnel plot analysis, which they found did not suggest evidence of publication
bias.
Figure 28. Prospective vs. retrospective studies.
The diamonds show the results of random effects meta-analysis.
There is substantial evidence that journals are rejecting and
delaying the publication of positive studies, for example by accepting a paper
for review, holding it for some time, and then rejecting it without review321,322.
One group performed prophylaxis and early treatment studies, with only the
less positive study being formally published to date148,152, suggesting a negative publication bias. Dr. Eli
Schwartz's269 double blind RCT was rejected without review by The
Lancet and Clinical Infectious Diseases323.
Authors of Efimenko do not plan to submit the very positive results
to a journal, and have self-censored the conference publication, providing
further evidence of a negative publication bias.
Trials with pending and possibly delayed publication often involve researchers
that may be restricted due to politics — publishing positive results may
be incompatible with continued employment, whereas negative results can
receive priority treatment at certain well-known journals, support the
positions of employers or funding organizations, and receive substantial
press.
For more details of censorship and negative publication bias in ivermectin
research see325-327.
Table 4 shows the reported results of physicians that use early
treatments for COVID-19, compared to the results for a non-treating physician
(this physician reportedly prescribed early treatment for themself, but not
for patients328). The treatments used vary between physicians. Almost
all report using ivermectin and/or HCQ, and most use additional treatments in
combination.
These results are subject to selection and ascertainment
bias and more accurate analysis requires details of the patient populations
and followup, however results are consistently better across many teams, and consistent
with the extensive controlled trial evidence that shows a significant
reduction in risk with many early treatments, and improved results with the use of
multiple treatments in combination.
| LATE TREATMENT | ||||||
| Physician / Team | Location | Patients | HospitalizationHosp. | MortalityDeath | ||
| Dr. David Uip (*) | Brazil | 2,200 | 38.6% (850) | Ref. | 2.5% (54) | Ref. |
| EARLY TREATMENT - 40 physicians/teams | ||||||
| Physician / Team | Location | Patients | HospitalizationHosp. | ImprovementImp. | MortalityDeath | ImprovementImp. |
| Dr. Roberto Alfonso Accinelli 0/360 deaths for treatment within 3 days |
Peru | 1,265 | 0.6% (7) | 77.5% | ||
| Dr. Mohammed Tarek Alam patients up to 84 years old |
Bangladesh | 100 | 0.0% (0) | 100.0% | ||
| Dr. Oluwagbenga Alonge | Nigeria | 310 | 0.0% (0) | 100.0% | ||
| Dr. Raja Bhattacharya up to 88yo, 81% comorbidities |
India | 148 | 1.4% (2) | 44.9% | ||
| Dr. Flavio Cadegiani | Brazil | 3,450 | 0.1% (4) | 99.7% | 0.0% (0) | 100.0% |
| Dr. Alessandro Capucci | Italy | 350 | 4.6% (16) | 88.2% | ||
| Dr. Shankara Chetty | South Africa | 8,000 | 0.0% (0) | 100.0% | ||
| Dr. Deborah Chisholm | USA | 100 | 0.0% (0) | 100.0% | ||
| Dr. Ryan Cole | USA | 400 | 0.0% (0) | 100.0% | 0.0% (0) | 100.0% |
| Dr. Marco Cosentino vs. 3-3.8% mortality during period; earlier treatment better |
Italy | 392 | 6.4% (25) | 83.5% | 0.3% (1) | 89.6% |
| Dr. Jeff Davis | USA | 6,000 | 0.0% (0) | 100.0% | ||
| Dr. Dhanajay | India | 500 | 0.0% (0) | 100.0% | ||
| Dr. Bryan Tyson & Dr. George Fareed | USA | 20,000 | 0.0% (6) | 99.9% | 0.0% (4) | 99.2% |
| Dr. Raphael Furtado | Brazil | 170 | 0.6% (1) | 98.5% | 0.0% (0) | 100.0% |
| Rabbi Yehoshua Gerzi | Israel | 860 | 0.1% (1) | 99.7% | 0.0% (0) | 100.0% |
| Dr. Heather Gessling | USA | 1,500 | 0.1% (1) | 97.3% | ||
| Dr. Ellen Guimarães | Brazil | 500 | 1.6% (8) | 95.9% | 0.4% (2) | 83.7% |
| Dr. Syed Haider | USA | 4,000 | 0.1% (5) | 99.7% | 0.0% (0) | 100.0% |
| Dr. Mark Hancock | USA | 24 | 0.0% (0) | 100.0% | ||
| Dr. Sabine Hazan | USA | 1,000 | 0.0% (0) | 100.0% | ||
| Dr. Mollie James | USA | 3,500 | 1.1% (40) | 97.0% | 0.0% (1) | 98.8% |
| Dr. Roberta Lacerda | Brazil | 550 | 1.5% (8) | 96.2% | 0.4% (2) | 85.2% |
| Dr. Katarina Lindley | USA | 100 | 5.0% (5) | 87.1% | 0.0% (0) | 100.0% |
| Dr. Ben Marble | USA | 150,000 | 0.0% (4) | 99.9% | ||
| Dr. Edimilson Migowski | Brazil | 2,000 | 0.3% (7) | 99.1% | 0.1% (2) | 95.9% |
| Dr. Abdulrahman Mohana | Saudi Arabia | 2,733 | 0.0% (0) | 100.0% | ||
| Dr. Carlos Nigro | Brazil | 5,000 | 0.9% (45) | 97.7% | 0.5% (23) | 81.3% |
| Dr. Benoit Ochs | Luxembourg | 800 | 0.0% (0) | 100.0% | ||
| Dr. Ortore | Italy | 240 | 1.2% (3) | 96.8% | 0.0% (0) | 100.0% |
| Dr. Valerio Pascua one death for a patient presenting on the 5th day in need of supplemental oxygen |
Honduras | 415 | 6.3% (26) | 83.8% | 0.2% (1) | 90.2% |
| Dr. Sebastian Pop | Romania | 300 | 0.0% (0) | 100.0% | ||
| Dr. Brian Proctor | USA | 869 | 2.3% (20) | 94.0% | 0.2% (2) | 90.6% |
| Dr. Anastacio Queiroz | Brazil | 700 | 0.0% (0) | 100.0% | ||
| Dr. Didier Raoult | France | 8,315 | 2.6% (214) | 93.3% | 0.1% (5) | 97.6% |
| Dr. Karin Ried up to 99yo, 73% comorbidities, av. age 63 |
Turkey | 237 | 0.4% (1) | 82.8% | ||
| Dr. Roman Rozencwaig patients up to 86 years old |
Canada | 80 | 0.0% (0) | 100.0% | ||
| Dr. Vipul Shah | India | 8,000 | 0.1% (5) | 97.5% | ||
| Dr. Silvestre Sobrinho | Brazil | 116 | 8.6% (10) | 77.7% | 0.0% (0) | 100.0% |
| Dr. Unknown | Brazil | 957 | 1.7% (16) | 95.7% | 0.2% (2) | 91.5% |
| Dr. Vladimir Zelenko | USA | 2,200 | 0.5% (12) | 98.6% | 0.1% (2) | 96.3% |
| Mean improvement with early treatment protocols | 238,381 | HospitalizationHosp. | 94.4% | MortalityDeath | 94.9% | |
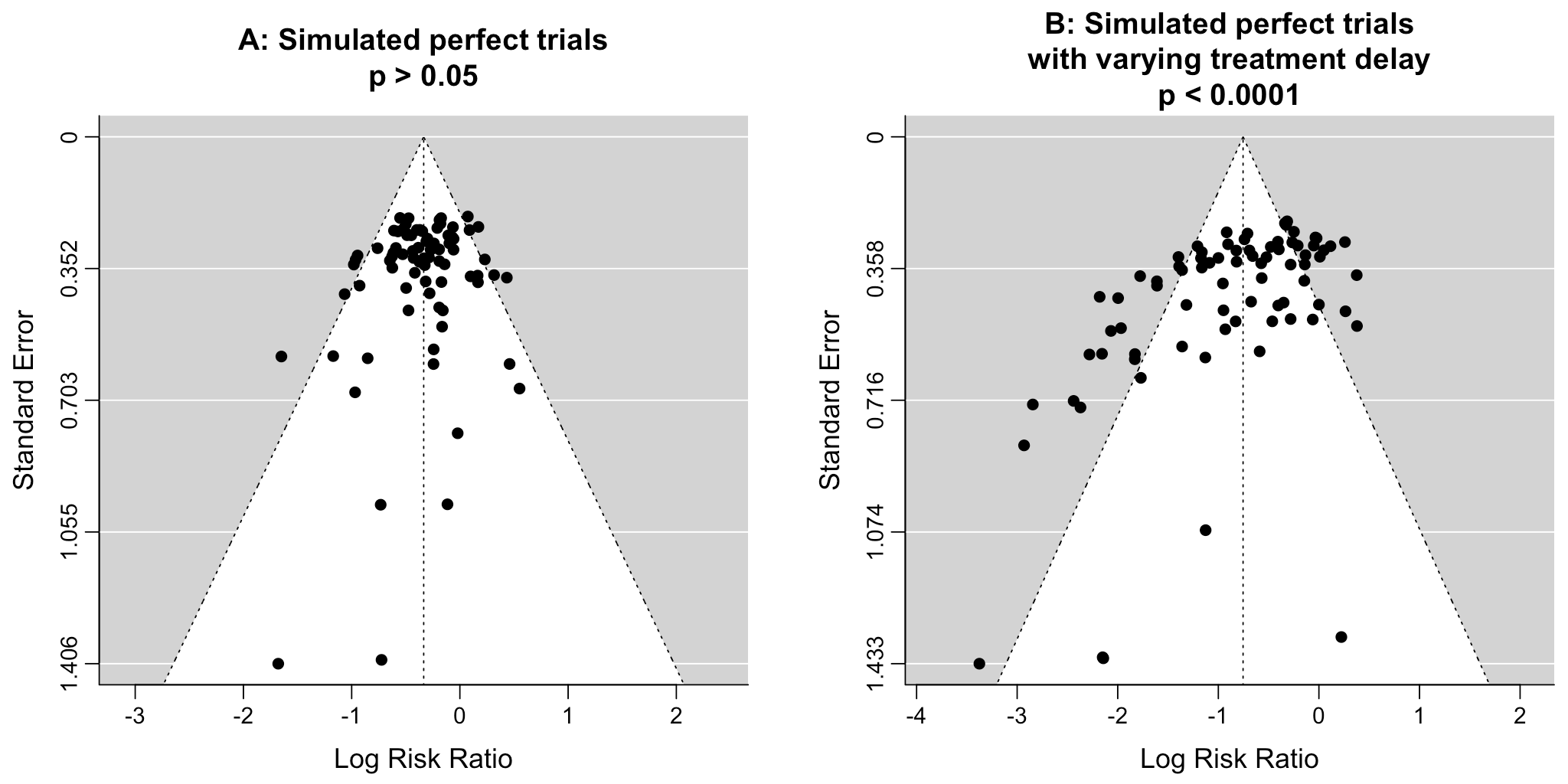
Funnel
plots have traditionally been used for analyzing publication bias. This is
invalid for COVID-19 acute treatment trials — the underlying assumptions
are invalid, which we can demonstrate with a simple example. Consider a set of
hypothetical perfect trials with no bias. Figure 29 plot A
shows a funnel plot for a simulation of 80 perfect trials, with random group
sizes, and each patient's outcome randomly sampled (10% control event
probability, and a 30% effect size for treatment). Analysis shows no asymmetry
(p > 0.05). In plot B, we add a single typical variation in COVID-19 treatment
trials — treatment delay. Consider that efficacy varies from 90% for
treatment within 24 hours, reducing to 10% when treatment is delayed 3 days.
In plot B, each trial's treatment delay is randomly selected. Analysis now
shows highly significant asymmetry, p < 0.0001, with six variants of
Egger's test all showing p < 0.05329-336.
Note that these tests fail even though treatment delay is uniformly
distributed. In reality treatment delay is more complex — each trial has
a different distribution of delays across patients, and the distribution
across trials may be biased (e.g., late treatment trials may be more common).
Similarly, many other variations in trials may produce asymmetry, including
dose, administration, duration of treatment, differences in SOC,
comorbidities, age, variants, and bias in design, implementation, analysis,
and reporting.
Figure 29. Example funnel plot analysis for simulated perfect trials.
Pharmaceutical drug trials often have conflicts of interest
whereby sponsors or trial staff have a financial interest in the outcome being
positive. Ivermectin for COVID-19 lacks this because it is off-patent, has
many manufacturers, and is very low cost. In contrast, most COVID-19
ivermectin trials have been run by physicians on the front lines with the
primary interest of finding the best methods to save human lives and minimize
the collateral damage caused by COVID-19. While pharmaceutical companies are
careful to run trials under optimal conditions (for example, restricting
patients to those most likely to benefit, only including patients that can be
treated soon after onset when necessary, ensuring accurate dosing), many
ivermectin trials do not represent the optimal conditions for efficacy.
Two ivermectin trials to date involve very large financial
conflicts of interest143,147 —
companies closely involved with the
trial or organizers stand to lose billions of dollars if ivermectin efficacy
becomes more widely known. The design of these trials favors producing a null
outcome as detailed in143,147. Note that biasing
an RCT to produce a false positive result is difficult (suppressing adverse
events is relatively easy337), but biasing a trial to produce a
false negative result is very easy — for example, in a trial of an
antiviral that works within the first 24 hours of symptom onset, trial
organizers only need to avoid treating people within the first 24 hours; or
with a disease like COVID-19, organizers only need to select a low-risk
population where most people recover quickly without treatment. We note that,
even under the very suboptimal designs, these trials produced positive
results, although without statistical significance.
Other treatments
may reduce the efficacy of ivermectin, for example dexamethasone may interfere
with the pharmacokinetics of ivermectin, significantly reducing plasma
concentration and efficacy338.
Several major trials have
been designed in a way that favors finding no effect, with a number of methods
including late treatment, selecting low-risk patients, fasting administration,
very high conflict of interest medication sourcing, and dosing below current
clinical practice. For discussion see339. One patient reported
their experience with one of the remote outpatient ivermectin/fluvoxamine
trials: they were offered enrollment 7 days after symptoms (receipt of
medication would be even later), were offered $400 to participate, and
reportedly target healthy people340. Details
of issues with several trials are included in the study notes.
The 105 studies are from 95 independent
research teams. 5 studies compare against
other treatments rather than placebo. Currently ivermectin shows better
results than these other treatments, however ivermectin may show greater
improvement when compared to placebo. 18 of
105 studies combine treatments, for example
ivermectin + doxycycline. The results of ivermectin alone may differ.
5 of 52 RCTs
use combined treatment, three with doxycycline, and one with iota-carrageenan.
2 of 105 studies
currently have minimal
published details available.
Summary statistics from
meta analysis necessarily lose information. As with all meta analyses, studies
are heterogeneous, with differences
in treatment delay, treatment regimen, patient demographics, variants,
conflicts of interest, standard of care, and other factors. We provide analyses for specific
outcomes and by treatment delay, and we aim to identify key characteristics in
the forest plots and summaries. Results should be viewed in the context of
study characteristics.
Some analyses classify treatment based on early or late
administration, as done here, while others distinguish between mild, moderate,
and severe cases. Viral load does not indicate degree of symptoms — for
example patients may have a high viral load while being asymptomatic. With
regard to treatments that have antiviral properties, timing of treatment is
critical — late administration may be less helpful regardless of
severity.
Details of treatment delay per patient is often not available.
For example, a study may treat 90% of patients relatively early, but the
events driving the outcome may come from 10% of patients treated very late.
Our 5 day cutoff for early treatment may be too conservative, 5 days may be too late in many cases.
Comparison across treatments is confounded by differences in
the studies performed, for example dose, variants, and conflicts of interest.
Trials with conflicts of interest may use designs better suited to the
preferred outcome.
In some cases, the most serious outcome has very few events,
resulting in lower confidence results being used in pooled analysis, however
the method is simpler and more transparent. This is less critical as the
number of studies increases. Restriction to outcomes with sufficient power may
be beneficial in pooled analysis and improve accuracy when there are few
studies, however we maintain our pre-specified method to avoid any
retrospective changes.
Studies show that combinations of treatments can be highly
synergistic and may result in many times greater efficacy than individual
treatments alone108,110,115,118,188,204-215 .
Therefore standard of care may be critical and benefits may diminish or
disappear if standard of care does not include certain treatments.
This real-time analysis is constantly updated based on
submissions. Accuracy benefits from widespread review and submission of
updates and corrections from reviewers. Less popular treatments may receive
fewer reviews.
No treatment or intervention is 100% available and
effective for all current and future variants. Efficacy may vary significantly
with different variants and within different populations. All treatments have
potential side effects. Propensity to experience side effects may be predicted
in advance by qualified physicians. We do not provide medical advice. Before
taking any medication, consult a qualified physician who can compare all
options, provide personalized advice, and provide details of risks and
benefits based on individual medical history and situations.
Typical meta analyses involve subjective selection criteria,
effect extraction rules, and study bias evaluation, which can be used to
generate a preferred outcome. In order to avoid bias we include all studies
and use a pre-specified method to extract results from all studies, in
addition to presenting results for higher-quality studies after exclusions.
Results to date are overwhelmingly positive, consistent, and insensitive to
potential selection criteria, effect extraction rules, and/or bias evaluation.
Additional meta analyses confirming the effectiveness of ivermectin can be
found in Kory, Lawrie, Bryant, Nardelli, Hariyanto, Ragó .
Kory et al. also review epidemiological data and provide suggested
treatment regimens.
The evidence supporting ivermectin for COVID-19 far exceeds the
typical amount of evidence used for the approval of treatments. Lee shows that only 14% of the guidelines of the Infectious Diseases
Society of America were based on RCTs. Table 5 and Table 6 compare the amount of evidence for ivermectin compared to
that used for other COVID-19 approvals, and that used by WHO for the approval
of ivermectin for scabies and strongyloidiasis. Table 7 compares US
CDC recommendations for ibuprofen and ivermectin.
| Indication | Studies | Patients | Status |
| Strongyloidiasis374 | 5 | 591 | Approved |
| Scabies374 | 10 | 852 | Approved |
| COVID‑19 | 105 | 220,423 | Pending |
| COVID‑19 RCTs | 52 | 17,642 |
| Medication | Studies | Patients | Improvement | Status |
| Molnupiravir (UK) | 1 | 775 | 50% | Approved |
| Budesonide (UK) | 1 | 1,779 | 17% | Approved |
| Remdesivir (USA EUA) | 1 | 1,063 | 31% | Approved |
| Casiri/imdevimab (USA EUA) | 1 | 799 | 66% | Approved |
| Ivermectin evidence | 105 | 220,423 | 60% [52‑67%] | Pending |
SARS-CoV-2 infection and replication involves a complex
interplay of 100+ host and viral proteins and other
factors28-35, providing many therapeutic
targets.
Over 9,000 compounds have been predicted to reduce COVID-19
risk36, either by directly
minimizing infection or replication, by supporting immune system function, or
by minimizing secondary complications.
Figure 30 shows an overview of the results for ivermectin
in the context of multiple COVID-19 treatments, and Figure 31 shows a plot
of efficacy vs. cost for COVID-19 treatments.
Figure 30.
Scatter plot showing results within the context of multiple COVID-19 treatments.
Diamonds shows the results of random effects meta-analysis.
0.6% of 9,000+ proposed treatments show efficacy375.
Figure 31. Efficacy vs. cost for COVID-19 treatments.
Ivermectin is an effective treatment for COVID-19. Treatment
is more effective when used early.
Meta analysis using the most serious
outcome shows 61% [50‑69%] and 85% [77‑90%] lower risk for early
treatment and prophylaxis, with similar results for
higher quality studies,
primary outcomes, peer-reviewed studies, and for
RCTs.
Significantly lower risk is seen for mortality, ventilation, ICU admission, hospitalization, recovery, cases, and viral clearance.
All remain significant for higher quality studies.
64 studies
from 58 independent teams
in 27 different countries
show significant improvements.
Results are very robust — in
worst case exclusion sensitivity analysis 63 of 105 studies must be
excluded to avoid finding statistically significant efficacy.
Optimal use of ivermectin may involve synergy with combined treatments,
administration taking into account the lipophilic nature, and sublingual,
spray, or inhaled formulations for direct treatment to the respiratory tract.
Pharmacokinetics show significant inter-individual variability1.
Injectable formulations may reduce variability and provide much faster onset
of action116.
Liposomal formulations show increased antiviral activity and lower
cytotoxicity111.
Synergistic results are seen with polytherapy108,110,115 .
Efficacy varies depending on the manufacturer2, underdosed
and contaminated ivermectin is common376-379,
and fake tablets with no active ingredient have been
reported349.
As Scott Alexander says:
"if you say anything in favor of ivermectin you will be cast out of
civilization and thrown into the circle of social hell reserved for Klan
members and 1/6 insurrectionists. All the health officials in the world will
shout 'horse dewormer!' at you and compare you to Josef Mengele." The
extreme politicization means we can only evaluate the data directly.
With 105 controlled studies,
52 RCTs, and extensive supporting evidence, few
people have the time and experience to analyze all or most of the evidence.
However, the PRINCIPLE trial146 provides a single large
trial showing efficacy. Despite being perhaps the most biased trial, with
extreme bias against showing efficacy in the design, operation, analysis, and
reporting, authors failed to eliminate the efficacy and hid the results for
600 days (810 days from
the expected announcement time, which resulted in a pause and continuation
with even greater bias).
PRINCIPLE showed 36% lower ongoing persistent COVID-19 specific
symptoms, p<0.0001146, and the primary recovery outcome
shows superiority of ivermectin with significantly faster recovery and a
probability of superiority > 0.999. While authors make an unprecedented claim
that the results are not clinically relevant, 2 days faster recovery and 36%
lower long COVID are both highly clinically relevant. Moreover, from all
172 treatments we cover, improved recovery is very
significantly associated with lower mortality, p < 0.0000000000001, as shown in Figure 32. These
highly positive results are despite very late treatment, a relatively low-risk
population, and poor administration — based on analysis of all trials
we expect significantly better results with recommended usage.
Figure 32. Improved recovery is associated with lower mortality. Meta-regression across 172 treatments.
| PRINCIPLE | 36% lower ongoing persistent COVID-19 specific symptoms, p<0.0001146. The primary outcome shows superiority of ivermectin with significantly faster recovery and a probability of superiority > 0.999. |
| TOGETHER | "There is a clear signal that IVM works in COVID patients.. that would be significant if more patients were added.." - co-principal investigator143. |
| ACTIV‑6 | 99%, 98%, 97% superiority for time unwell, progression @14,7 days144 (note: the clinical progression results were modified in the journal version, with no explanation for over 900 days, and the 600µg/kg results also differ without explanation). |
| COVID‑OUT | 61% lower hospitalization (ivermectin vs. placebo, unreported)145. Authors detail why the hypoxemia results are unusable, however analysis of the data shows that the ER results are similarly uninformative and do not appear to be related to symptoms. |
The team referenced in this article is unreliable.
Dr. Kyle Sheldrick posted a schedule A statement as a result of a defamation
lawsuit admitting to false and defamatory claims regarding one of the world's
most highly published and respected critical care physicians380;
Dr. Nick Brown has called for trials for crimes against humanity for
scientists that "tried to scam the world with their fake treatments"
including vitamin D381,382.
Gideon Meyerowitz-Katz has posted many false claims detailed below383.
Update: authors indicated that their data would be available "soon" as
of Sep 14, 2021, however it has not been released over 1,300 days
later384,
therefore it is not possible to analyze their methods regarding
ivermectin research in detail.
However, Dr. Sheldrick posted false
and defamatory accusations regarding a highly respected physician that has
saved countless lives before and during the pandemic. In this case, detailed
methods were published, revealing highly flawed analysis, and a basic
misunderstanding of statistics, as detailed by multiple statisticians385,386.
Author deleted the blog post.
Further, we
note that the team's disregard for major issues with the Together Trial, ACTIV-6, López-Medina et al., and Beltran Gonzalez et al. suggest substantial
bias.A BBC article raises questions due to data issues in some
studies, based on an analysis from a team of researchers. One of the
researchers reports that data in some trials could have been manipulated,
while noting that human error can not be ruled out. Others in the team
directly accuse authors of malfeasance. Regardless of the cause, concern over
these studies is valid. Currently, 2 studies have been retracted, one was
withdrawn by a preprint server, and another has been reported as pending
retraction, although the journal reports that no retraction is pending. None
of these studies are in our analysis.
Existence of some lower quality studies is typical in large
evidence bases. The percentage of studies with issues is not greater than
reported averages, and is not close to removing evidence of efficacy (and may
actually improve evidence as detailed below). We performed an absolute worst
case sensitivity analysis, where positive studies are excluded in order of
the effect size, with the largest effect first.
60%, or 63 of 105 studies must be excluded to avoid
finding statistically significant efficacy (this is in addition to the four
papers not in this analysis).
The summary statistics from meta analysis necessarily obscure
most of the information in the evidence base. For those that have read all of
the research, knowledge of efficacy is supported by extensive additional
information, including for example relationships between outcomes within a
study, dose-response relationships within and across studies, treatment
delay-efficacy relationships within and across studies, variant-efficacy
relationships, etc. Notably, removal of Elgazzar, Samaha, and Niaee improve
the treatment delay-efficacy and dose-response relationships and may further
increase confidence when considering all information.
Concerns about Cadegiani, Carvallo, Carvallo (B), Carvallo (C) have also been
reported. All of these studies are excluded in our exclusion
analysis.
| Studies | Prophylaxis | Early treatment | Late treatment | Patients | Authors | |
| With GMK/BBC exclusionsw/GMK/BBC exclusions | 70 | 84% [73‑91%] | 69% [61‑76%] | 48% [32‑60%] | 202,821 | 831 |
| RCTs w/GMK/BBC exc.RCTs w/GMK/BBC exc. | 39 | 89% [57‑97%] | 65% [53‑74%] | 34% [14‑50%] | 12,977 | 532 |
| Percentage improvement with ivermectin treatment after exclusion of all studies reported by this team | ||||||
We note that, while malfeasance cannot be ruled out, reported
concerns may also be caused by typos, data collection errors not affecting
analyzed outcomes, and expected results from multiple tests. Authors, without
any prior registration or statistical analysis plan, perform thousands of
statistical tests across data in the studies and report results without
correcting for multiple tests. For example, reporting the occurrence of a 1
in 1,000 event as evidence of randomization failure, while performing more
than this number of tests across studies.
This group often dismisses studies based on an arbitrary
statistical significance threshold for a specific outcome, a misunderstanding
of statistics387, and indefensible as a pre-filter in meta
analysis.
This group has made many claims unsupported by the data. For
Niaee, one author claimed the study "made a HUGE difference". It has
no effect on early treatment or prophylaxis. For late treatment, which
is not recommended, the change was relatively minor. For Elgazzar, the author
claimed that it could be "the most consequential medical fraud ever
committed". There was almost no difference in our analysis after removing
this paper (excluding 1 of 108
studies has very little effect,
and the exclusion actually improves the treatment delay-response
relationship).
Statements by the group suggest significant bias. The main
author first referred to ivermectin as "something else to debunk" in December
2020, and later as a "horse dewormer". Another group member has called for
charging scientists that recommend vitamin D with "crimes against humanity".
The group has made claims about all ivermectin evidence based
on the existence of some studies with issues. It is inappropriate to
generalize about the entire group of 1206
scientists and researchers based on the
mistakes or actions of a few individuals.
This group has focused on finding issues in papers reporting
large positive effects, which introduces a significant bias. Notably, the few
studies that contribute most to minimizing the effects in meta analysis
include studies with very high conflicts of interest and many reported
protocol violations and data issues, however this group disregards all of
these issues.
The article claims "The largest and highest quality
ivermectin study published so far is the Together trial" which "found
no benefit", however this study has not been published, is one of the lowest quality trials with many documented
design, execution, and analysis issues, has extremely high conflicts of
interest, there is a history of inaccurate
reporting prior to publication for a previous treatment in the same
trial, and the trial actually reported 18% lower mortality (not statistically
significant).
The article reports that 26 studies were examined, however
there are 108 studies, authors have
not reported their results for all 26, and authors have not provided their
data after repeated requests. Currently they have not even provided a list of
the 26 studies.
The group has an excessive focus on RCTs, which have a
fundamental bias against finding an effect for interventions like ivermectin
that are widely known and easily available — patients that believe they
need treatment are more likely to decline participation and take the
treatment388 (this does not apply to the typical pharmaceutical
trial of a new drug that is otherwise unavailable and unfamiliar).
The main author of the group is also against vitamin D. Of the
126 vitamin D COVID-19 treatment
studies, author suggests only one trial is worth looking at389.
This gives us a simple case to examine potential bias. Murai is a
small trial providing no statistically significant effects (mortality p
= 0.43, other outcomes are positive while also not significant). Author
acknowledges that the trial is too small for a conclusion. More importantly,
this trial provides no information about whether vitamin D reduces the risk of
a serious COVID-19 case, because the patients in this trial already had a
serious COVID-19 case (90% already on oxygen treatment at baseline). Author
does not mention this. The trial also has poorly matched arms in terms of
gender, ethnicity, hypertension, diabetes, and baseline ventilation, all
favoring the control group. Further, this study uses an inappropriate form of
vitamin D — cholecalciferol. In reality physicians would use calcifediol
or calcitriol with late stage treatment, because they avoid a very long delay
for conversion. We are unaware of a reason to use cholecalciferol in this case
(other than to produce a null result). In summary, author's chosen study is
the study providing the least useful information from the
126 vitamin D treatment studies to
date, suggesting biased analysis.
We fully support this team's effort to clean up the evidence
base. This is extremely valuable and improves the integrity of the evidence
base (and the accuracy if done equally for all studies). We hope this or
other teams can do the same for all treatments. However the analysis plan
should be published, details of all tests should be provided, results should
be corrected for multiple testing, results for all studies and tests should
be provided, and equal attention should be given to studies with
non-statistically significant results, especially those with major reported
data issues that have been disregarded by this team (for example data
suggesting substantial protocol violations including confounding by time in
Reis and control arm use of treatments in López-Medina).
For coverage of other errors in the BBC article, and
illumination of the stark contrast between Dr. Lawrie's response to the BBC
before publication and what they chose to report, see BiRD Group, Elijah, Lawrie (B), Campbell .
More details can be found in the following response regarding
the main author of this group.
On September 6, 2021, author is on video saying
"what this web site does is it goes through all of those 10 things, finds
the positive one, and only reports the positive one ... they'll pick a number
that is the lowest number"394
@46:48. This is false, we report individual outcome analyses, and for pooled results we
use the most serious outcome with a detailed protocol. Notably, author knows
this is false, having posted the protocol on Twitter a month earlier.
Moreover, in most cases there could be no ambiguity on the most serious
outcome even without a detailed protocol. At the time of author's
statement, the most serious outcome was actually the worst of multiple
reported outcomes 26% of the time.
Author indicated their data would be released "soon"
on Sep 14, 2021. The data was used for conclusions in the BBC and BMJ along
with a message that data transparency is needed. No data has been released
over 1,300 days later384.
TLDR
As a quick way to assess
reliability, consider that author describes the Together Trial as "incredibly
well-done" and a “masterpiece
of science". The trial actually reported multiple impossible numbers,
has refused to release data despite pledging to do so, has extreme conflicts
of interest, and had blinding failure, randomization failure, and multiple
protocol violations as detailed below.
Author similarly disregards major issues with many other trials, including ACTIV-6, López-Medina et al., and Beltran Gonzalez et al. This
suggests substantial bias.
Incorrect, misleading, hyperbolic, and unsupported statements
have been made by an influential anti-treatment Twitter personality,
journalist, and PhD student known for defending
Monsanto Roundup against carcinogenic claims (later settled for $US 11
billion). Author is notable as the only known researcher that reports having
read a majority of the 108
(including retracted) studies, but does not find the evidence to be positive.
However, their opinion appears to have been formed before reading the studies
— they first referred to ivermectin as "something else to
debunk". We note that the author has made valuable contributions
identifying significant issues with some studies, which has helped to improve
the quality of the ivermectin evidence base, and has improved the
dose-response and treatment delay-response relationships.
Analysis with GMK's recommended exclusions can be found in the
supplementary data, which shows 46% [33‑56%] improvement, p = 0.0000000083.
Author has been paid for writing anti-treatment articles, and
has also referred to ivermectin as a "horse dewormer". Author has
experienced personal tragedy with multiple family members having died of
COVID-19, which may introduce a bias against acknowledging errors in treatment
advice.
Author's attempt to discredit the scientists performing
ivermectin research centers on the false assertion that excluding a small
number of lower quality trials results in a negative outcome. It should be
clear from the forest plot that this is not possible, but we can be more
specific. We perform a worst case sensitivity analysis, where positive studies
are excluded in order of the effect size, with the largest effect first. How
many studies do we need to exclude before the meta analysis RR has a
confidence interval exceeding 1.0?
60%, or 63 of 105 studies must be excluded to avoid
finding statistically significant efficacy. As with all data in this
paper, this analysis will automatically update as the evidence base evolves.
Also note that this is after exclusion of withdrawn papers - one has never
been in this analysis, the second was removed on the same day it was
withdrawn, and the other two were removed in advance of retraction based on
author's notification that retraction is pending (only one has been retracted,
the journal for Niaee et al. has reported that no retraction is
pending).
Author claims that we include several papers that are already
excluded in the 11 exclusion analyses.
Author claims that there is a greater percentage of low quality
studies for ivermectin and COVID-19 compared to other treatments. This is
unsupported for such a large evidence base, and does not match previous
studies.
Author often makes a basic error by equating positive effects
that are not statistically significant at a specific level with "no effect",
a misunderstanding of statistics387. For example, if a study
reports 50% improvement with a p value of 0.1, we cannot say that the
study shows the treatment is ineffective, or in the words of the author
shows "no benefit at all". Author repeatedly makes false claims in this
way.
On Sep 14, 2021, author indicated that their team had
reviewed about 30 ivermectin studies and their data would be available soon,
however it has not been released three years
later.
Author appears to favor pharmaceutical company
affiliated/operated trials. For example, the author has no problem with the
lack of IPD for many pharmaceutical affiliated COVID-19 trials that support
the author's treatment positions, yet considers the lack of IPD in a positive
ivermectin trial to be problematic. Author believes the pharmaceutical
affiliated Together Trial is the highest quality trial so far, yet not only
have the authors declined to release IPD that they previously pledged to
release, there was not even a preprint when GMK made the statement, and the
trial has many critical and serious
flaws, extremely high conflicts of interest, and a history of inaccurate reporting prior to publication
for another treatment arm. GMK has subsequently published a paper with one of
the original co-lead's of the Together Trial (who later joined the trial
DSMC).
Author has disregarded treatment delay in
analysis, which results in incorrect conclusions. For example, author claims
that the RECOVERY trial proved that another treatment is not effective, and
would provide definitive data if the same was done for ivermectin. The trial
provided valuable data on very late use (9 days after symptoms) with an
excessively high dose and very late stage patients. However, it did not
provide information on early treatment. Oseltamivir, for example, is generally
only considered effective for influenza when used within 0-36 or 0-48 hours190,191. Paxlovid was tested with a maximum of 3 days from
symptom onset (the mean delay is unknown). For ivermectin, author believes the
PRINCIPLE trial will provide strong data on efficacy, however this trial
includes low risk patients less than 15 days from symptom onset, and may only
provide information on late treatment in a low risk population with lower risk
variants. Figure 33 shows a mixed-effects meta-regression for
efficacy as a function of treatment delay in COVID-19 studies from 172
treatments. Efficacy declines rapidly with treatment delay.
Figure 33. GMK believes that results for
treatment delayed 9 days from symptom onset provides definitive information on
treatment efficacy. However early treatment is critical for
antivirals, as shown with antivirals for other
respiratory diseases, and in meta-regression of studies from 172 COVID-19
treatments.
Author has an unwarranted focus on a specific outcome
(mortality) and a specific subset of trials (RCTs). This would be reasonable
in many cases when sufficient high-quality data is available, however this is
not the case for off-patent COVID-19 treatment trials, where RCTs often
involve delayed treatment, low-risk patients where mortality is rare, or very
high conflicts of interest. Widely accepted and
effective (for specific variants) treatments like casirivimab/imdevimab,
bamlanivimab, and sotrovimab were all approved without statistically
significant mortality benefits. Other outcomes are also important —
accelerating viral clearance, and reducing cases, hospitalization, ICU
admission, ventilation, etc. are all very valuable, for example reducing
serious "long COVID" problems, reducing transmission of the virus, and
reducing the burden on the healthcare system. These outcomes are also likely
to correlate with reduced mortality among larger or higher-risk populations.
We note that there is extensive evidence for the mortality outcome when not
restricting to RCTs. RCTs have mostly been run with relatively low risk
populations where mortality is low, leading to limited statistical
significance. However RCTs are inherently biased towards low mortality and
towards not finding an effect in this case — ivermectin is well-known to
be beneficial for COVID-19 and is easily available, therefore participants
that believe they may be at serious risk are more likely to decline
participation in the RCT and take the recommended medications. Patients that
do choose to participate are also more likely to have low adherence. This bias
of RCTs is likely to be even larger in locations where ivermectin is widely
used in the community and very easily obtained, which correlates with the
observed RCT results.
Author suggests that we have chosen the wrong outcome in some
cases. While mistakes are possible, for example we corrected errors with Espitia-Hernandez et al. and Jain et al., the claims made
suggest that the author has not read the studies and/or our protocol
carefully. Details are below. We note that the author disregards the
existence of the individual outcome
analyses and the primary outcome
analysis.
Most errors have not been corrected by the author over
three years later. Many false, misleading, and defamatory
statements continue to be available, highly-ranked in search results, and
highly influential. Other errors include:
•that excluding Elgazzar et al.
completely changes the results and could be "the most consequential
medical fraud ever committed". Excluding 1 of 108 studies has very little effect,
and the exclusion improves the treatment delay-response relationship.
•that Niaee et al. "made a HUGE
difference". It has no effect on early treatment or prophylaxis.
For late treatment, which is not recommended, the change was minor,
and the exclusion improves the treatment delay-response relationship.
•making basic errors suggesting very
superficial reading of studies, for example claiming the RR in Szente Fonseca
is the risk of being treated.
•making basic errors suggesting very
superficial reading of this paper, for example claiming that a result for
prophylaxis studies is based on the number of patients from all
studies.
•equating a high degree of COVID-19 in
a country partially adopting a treatment with a lack of efficacy,
disregarding obvious confounding such as heavily affected areas being more
likely to adopt treatment (analysis of results in regions or time periods
adopting treatment, while not equivalent to controlled studies, is more
informative and shows efficacy244,395-397).
•confusing heterogeneity due to dose,
treatment delay, etc. and due to bias.
•disregarding treatment delay to
dilute or obscure effects by including late treatment (author has also used
this method with other treatments).
•disregarding the existence of
specific outcome analyses, RCT analysis, and exclusion-based sensitivity
analysis.
•suggesting that efficacy over longer
periods is not possible because ivermectin has a half-life of "about a day".
Author disregards known efficacy for other conditions over much longer
periods, and mischaracterizes the half-life. Antiparasitic efficacy can
persist for several months after a single dose398. Plasma
half-life is longer in some studies, and significant plasma concentration can
persist for over 2 weeks in some patients399. More importantly,
ivermectin is highly lipophilic and may accumulate in the lung and other
tissues where concentrations may be many times higher400,401.
•misunderstanding funnel plot
analysis and explanations other than selective reporting (and providing no
evidence of unreported negative studies, while there is substantial evidence
of difficulty publishing positive studies321,322).
•suggesting that it is not reasonable
to combine evidence from mortality and hospitalization (for example), but
happily combining late treatment and early treatment in order to obscure
efficacy. If a treatment reduces disease severity requiring hospitalization,
reduced mortality in at-risk populations logically follows, whereas lack of
efficacy several days after onset can not be extrapolated to early treatment
— treatments for a viral infection are often less effective when
delayed.
•making serious claims about
individual studies without contacting authors (for example claiming patients
were excluded for reaching the endpoint too quickly in one study, whereas authors report
exclusions due to baseline negative status).
The cases where author suggests we have chosen the wrong
outcome indicate that the author has not read the studies and/or our protocol
carefully:
•suggesting that the risk of a good
outcome should be selectively used instead of the risk of a bad outcome
(author would like to do this when it reduces the effect size). This is similar
to using the risk of surviving instead of the risk of death. 99% survival
may only be a 4% improvement over 95% survival, but most people would
appreciate the 80% lower risk of death.
•suggesting that hospitalization time
should be used for symptomatic recovery in a study where discharge is based
on viral clearance (and only tested weekly).
•suggesting that a specific symptom
such as cough should be used (author would prefer a less positive result for
the study).
•suggesting that viral load is more
important than symptomatic results.
•suggesting that mortality should be
used in populations with zero mortality (for low-risk populations with no
mortality, reduction in mortality is not possible, this does not mean a
reduction in hospitalization, for example, is not valuable).
•suggesting that unadjusted results
should be used in a study where the adjustments clearly make a significant
difference (author wants to cherry-pick unadjusted cough results).
•suggesting that, for example, in a
study of viral load where all patients recover, it is not valuable if treated
patients recover faster (or are less likely to transmit the virus to
others).
•suggesting that study selected
outcomes should have priority rather than using a consistent pre-specified
protocol, disregarding the added bias and the fact that this actually
improves results for ivermectin (for example the very small event count
negative serious outcomes in Krolewiecki, Vallejos, and Buonfrate would no
longer have priority).
•suggesting that cough is a more
important symptom than low SpO2 or fever. Cough can persist for a
long time after more serious symptoms resolve, and persistent cough may be
caused by many conditions.
•suggesting that combined low dose
treatment results should be used in a study that had a combined
ivermectin/doxycycline arm (single dose ivermectin, 5 days doxycline) and an
ivermectin arm with treatment for 5 days.
We note that this personality has an extensive history of
incorrect advice, including for example:
•claiming that flu is more dangerous
than COVID-19
•claiming that SARS-CoV-2 is not
airborne
•claiming that it's impossible to
improve immune system functioning
•even believing and propagating a made
up story that claimed ivermectin overdose was causing gunshot victims to wait
at an ER
Author has taken a public position against early treatments for
COVID-19 since at least July 2020. Given this longstanding and influential
negative position, they may tend to view information with a negative filter
and confirmation bias, and may be reluctant to admit errors. They acknowledge
not having read all of the studies (and appear to have very superficially read
others). They submitted zero feedback to us, suggesting that they know their
comments are incorrect or that they have a motivation other than correcting
errors. Author claims that they could not contact us, however there are over
50 feedback links throughout this article. We also note that the author is not
open to critical feedback and routinely blocks Twitter users correcting
mistakes or expressing anything critical on their feed. Reports suggest that
the author also pre-emptively blocks people that have not even interacted with
them, but are connected to other users reporting on their errors. Author
ackowledges using a tool called MegaBlock that blocks all people that liked a
specific tweet.
The author is also against vitamin D. Of the
126 vitamin D COVID-19 treatment
studies, author suggests only one trial is worth looking at389.
This gives us a simple case to examine potential bias. Murai is a
small trial providing no statistically significant effects (mortality p
= 0.43, other outcomes are positive while also not significant). Author
acknowledges that the trial is too small for a conclusion. More importantly,
this trial provides no information about whether vitamin D reduces the risk of
a serious COVID-19 case, because the patients in this trial already had a
serious COVID-19 case (90% already on oxygen treatment at baseline). Author
does not mention this. The trial also has poorly matched arms in terms of
gender, ethnicity, hypertension, diabetes, and baseline ventilation, all
favoring the control group. Further, this study uses an inappropriate form of
vitamin D — cholecalciferol. In reality physicians would use calcifediol
or calcitriol with late stage treatment, because they avoid a very long delay
for conversion. We are unaware of a reason to use cholecalciferol in this case
(other than to produce a null result). In summary, author's chosen study is
one of least useful studies from the
126 studies to date, suggesting
biased analysis.
Based on many comments, author appears to focus on superficial
criteria such as typesetting and quality of writing. While many of the
studies have been performed by non-native English speakers with minimal
budgets, this does not imply the researchers are less reliable. Indeed, the
author is highly critical of the program used to create a graph, for example,
but is unable to see flaws in high budget high conflict of interest trials,
even when they prompt >100 scientists to write an open letter requesting
retraction220.
Three years later, the author has still
not contacted us, making content-free comments on Twitter such as calling us
"sh*tty". Other individuals pointing out errors with detailed and
careful feedback get similar treatment, such as being called a
"d*ckhead" and being blocked.
More details can be found in the BBC
response.
Feb 2, 2023 update: Scott acknowledges that his analysis
was incorrect, that the topic is outside his "expertise and competence
level", and that his self-and-GidMK-filtered subset of a 29 study subset
of 105 studies actually shows much stronger
efficacy than previously claimed. Scott further acknowledges several false and
defamatory claims, while standing by others. Scott acknowledges that the strongyloides
theory is not very strong. Scott now relies on publication bias to
discredit the 653
scientists reporting efficacy, without even reading many of their
studies.
For publication bias, author is saying that the statistically
significant positive studies were chance events, i.e., there are actually
>1,000 ivermectin studies, but there is an extremely strong bias towards
publishing only the positive studies.
This is in direct opposition to the evidence on publication bias. High profile
journals refuse to publish positive ivermectin studies, while negative
ivermectin studies are guaranteed acceptance, widespread press, and fame, just
as Scott has received fame for his negative article. As Scott said in November
2021, "if you say anything in favor of ivermectin you will be cast out
of civilization and thrown into the circle of social hell reserved for Klan
members and 1/6 insurrectionists. All the health officials in the world will
shout 'horse dewormer!' at you and compare you to Josef Mengele."
Ivermectin has the strongest negative publication bias we have ever seen.
Scott finally points at our overview of efficacy across
treatments, claiming that multiple effective treatments is proof of
publication bias. As if somehow the existence of several effective treatments
is impossible.
Scientists have identified over 2,000 compounds potentially
beneficial for COVID-19. It is trivial to disable SARS-CoV-2 in vitro,
hundreds of compounds do so, many with existing known and positive safety
records. What is the chance that none of these can safely reach the location
of SARS-CoV-2 infection? In the nasopharynx, oropharynx? Lung? Other tissues?
Is it really surprising that PVP-I for example, very effective
in vitro, can be applied to the nasopharynx/oropharynx in effective
concentrations, and is helpful, especially if used before infection spreads
further?
Are there really no inputs to the human system that improve
functioning of the immune system?
Does Scott really believe that paxlovid, casirivimab/imdevimab,
sotrovimab, tixagevimab/cilgavimab, bebtelovimab, ensovibep, molnupiravir, and
remdesivir are actually ineffective, all were approved in error because
hundreds of other studies were not published?
While Scott dismisses the work of over 10,500
scientists reporting statistically significant positive effects of low cost
treatments (over 600 for
ivermectin), he appears to have blind faith in trials having perhaps the
highest moral and financial conflicts in the history of medicine, while
simultaneously missing many critical issues (ACTIV-6, TOGETHER, COVID-OUT, PRINCIPLE) creating unreliable results, and signs of
efficacy despite best efforts to avoid it.
Extreme moral conflicts arise for authors and institutions that
played a critical role in the suppression of early treatments — they
share responsibility for the results of any mistakes that impacted policies.
The extreme financial conflicts come from authors and institutions associated
with companies where billions of dollars of profit relies on no effective
inexpensive treatments existing.
We challenge Scott to do a more serious analysis. For example:
examine all of the studies rather than only
28%; directly examine studies
rather than relying on a personality that thinks a study treating patients 9 days after onset is conclusive (a study
so extremely late that 17% were on ventilation/ECMO); take into account major
issues with studies like ACTIV-6, TOGETHER, COVID-OUT, and PRINCIPLE; and review the ~100 additional supporting papers for
understanding of the mechanisms of action, censorship, and other issues.
Previous response: For a much better and more thorough
analysis of Scott Alexander's essay, including numerous errors, extreme bias,
incorrect statistical analysis, contradictory standards, and failure to make
corrections, see the Potemkin Argument series. Part 21 illustrates the
potentially catastrophic result of humanity's difficulty in objectively
creating and evaluating scientific evidence related to critical world
problems.
See also
The analysis by SSC / Scott Alexander has a number of major issues.
For many other uncorrected errors in SSC's analysis, see
doyourownresearch.substack.com, twitter.com (E).
Analysis with SSC's recommended exclusions can be found in
the
supplementary data.
Update: after exclusions chosen by SSC,
exclusions by GMK, excluding all late treatment, and excluding all prophylaxis
studies, SSC found the results in Figure 34, showing statistically
significant efficacy of ivermectin with p = 0.04. The method for
computing this p value is not specified. We used the same event results
and performed random-effects inverse variance DerSimonian and Laird meta
analysis as shown in Figure 35, finding much higher significance with
p = 0.005. We note that the effect extraction appears biased against
ivermectin, choosing the excessive dose arm in Buonfrate, and using the
post-hoc exclusion in López-Medina. The Krolewiecki treatment count appears to
have been scaled for the different group sizes. We do not know where SSC's
Mahmud counts are from.
{kind=link}
Figure 34. SSC's analysis. SSC reports p = 0.04, with an unspecified method.
{kind=link}
Figure 35. Random-effects meta analysis per SSC's
chosen results, finding much higher significance.
Author appears to be against all treatments, labeling them all
"unorthodox" and "controversial", even those approved by western
health authorities, including casirivimab/imdevimab, bamlanivimab, sotrovimab,
and paxlovid. Update: author's original article still refers to all
treatments we follow as unorthodox and controversial, however they report that
they actually recommend fluvoxamine, paxlovid, casirivimab/imdevimab,
bamlanivimab/etesevimab, and sotrovimab, and suggest that they support all
western health authority approved treatments which additionally includes
remdesivir, budesonide, bebtelovimab, tixagevimab/cilgavimab, and
molnupiravir. Author also has positive comments for zinc (but reports there is
no proof). i.e., author appears to actually support at least 11 of the
172 treatments we follow. We note that the methodology is
the same for all treatments.
We encourage the author to at least direct readers to
government approved treatments, for which there are several in the author's country, and many
more in other countries
(including ivermectin). While approved treatments in a specific country may
not be as effective (or as inexpensive) as current evidence-based protocols
combining multiple treatments, they are better than dismissing everything as
"unorthodox". Elimination of COVID-19 is a race against viral
evolution. No treatment, vaccine, or intervention is 100% available and
effective for all variants — we need to embrace all safe and effective
means.
The third-party analysis that author references for the
strongyloides theory is confounded by treatment delay and dosage — the
high prevalence group has more early treatment trials and a higher average
dose, i.e., the analysis reflects the greater efficacy of early treatment and
the greater efficacy of higher dosage. More details can be found in the
strongyloides section.
Author refers to studies with positive but not statistically
significant results as "negative"239, or "[the]
original outcome would also have shown ivermectin not working"147, which are incorrect conclusions387.
Update: author believes this means we abandon statistical
significance. We do not know where this comes from — all of our results
report confidence intervals, and the first two words of this paper are
"statistically significant". What is incorrect is making a negative conclusion
based on an insignificant result. For example, if one study reports 50% lower
mortality without reaching statistical signifiance, this does not mean that
the treatment is useless. Consider if there are 10 studies all reporting ~50%
lower mortality, the combined evidence may be strong even if each individual
result is not statistically significant.
Author notes that: "if you say anything in favor of
ivermectin you will be cast out of civilization and thrown into the circle of
social hell reserved for Klan members and 1/6 insurrectionists",
suggesting an environment that may bias the information that the author sees,
and could unconsciously bias analysis. We note that similar environments
influence the design, operation, and publication of some existing (and many
upcoming) ivermectin trials.
Author looks at 29 of the 105
studies, which we note is much better than most commenters, but still ignores
the majority of studies, including the prophylaxis studies.
The author finds efficacy at p = 0.04 in their analysis
of 11 of the 29 studies they looked at. We note that simply looking at the
other 76 studies will result in much higher
confidence in efficacy. We also note that even at p = 0.04 with 11
independent studies, a rational risk-benefit analysis results in immediate
adoption into protocols (pending stronger data with other combinations of
treatments), and immediate collection of more data from sources without
conflicts of interest.
However, ultimately the author at least partially supports the
two prevailing theories that are commonly used by those against treatment.
These theories require disregarding extensive contradictory evidence:
The steps required to accept the no-significant-effect
outcome are extreme — one needs to find a reason to exclude most of the
studies, disregard the strong treatment-delay response relationship, and
disregard all prophylaxis studies. Even after this, the result is still
positive, just not statistically signficant. This does not support a negative
recommendation. Widely accepted and effective (subject to dependence on viral
variants) treatments like casirivimab/imdevimab, bamlanivimab, and sotrovimab
were all approved without statistically significant mortality benefits.
The steps required to accept the
strongyloides-mechanism-only conclusion are also extreme - we need to
disregard the majority of outcomes occuring before steroid use, and disregard
the strong treatment-delay response relationship which is contradictory.
Figure 27 shows analysis by strongyloides prevalence. The third-party
analysis referenced by the author is confounded by
treatment delay and dosage.
Author seems biased against believing any large effect size. We
note that large effect sizes have been seen in several COVID-19 treatments
approved by western health authorities, including paxlovid which the author is
very positive about, and also that better results may be expected when studies
combine multiple effective treaments with complementary mechanisms of action
(as physicians that treat COVID-19 early typically do). Update: author
confirms this bias but appears to disregard it for paxlovid.
Author is suspicious about a study based on the country of the
researchers, and also appears biased against non-native speakers, with
comments such as "unreadable" for one paper, compared to "written up
very nicely in real English" for another. Update: author confirms being
biased against certain countries.
Author calls a physician that has reported zero deaths and 5
hospitalizations with 2,400 COVID-19 patients "a crazy person" that
"put his patients on every weird medication he could think of".
Author disregards the dramatically higher mortality for Gamma
vs non-Gamma variants (aHR 4.73 [1.15-19.41]199), instead
concluding that higher mortality indicates fraud in one instance, while in
another instance assuming that the related confounding by time in the Together
Trial is not significant.
Author's review of the 29 studies appears relatively cursory,
for example author appears unaware that the ivermectin dosage is very
different in the ivermectin + doxycycline arm of Ahmed.
Author appears to accept the analysis and accusations of GMK as
correct, however that author is often
incorrect.
Author is concerned that we detail problems with
López-Medina, while correctly noting that the outcomes in this trial
are actually positive and in favor of ivermectin (while not statistically
significant in isolation).
Author is concerned that we specifically comment on
Reis, López-Medina. We note that it has been others that have
focused on these trials — we comment on them because they have received
special attention, including being held up as sole evidence overriding all
other trials, despite having major issues.
This study was withdrawn and
was removed from this analysis on the same day. There was no significant
change (excluding 1 of 108 studies
has very little effect, and the exclusion actually improves the treatment
delay-response relationship).
This study was removed
from this analysis within an hour of notification that it was pending
retraction. There was no significant change in the results, and the exclusion
improves the dose-response relationship.
This preprint was censored by the
original preprint host. Censors claim that the government treatment program,
which used approved medications and saved over 500 people from
hospitalization, was unethical. In part they also indicate that studies of
"the effects of a medication on a disease outcome" are outside the scope of
their site.
The author's response (not provided by the censors) can be
found here: twitter.com (F).
Author's provide the data and code for the study, and the results have been
independently verified.
This paper appears to
have been censored at the request of the journal's founding editor405. An external review is
mentioned but is not provided, and there is no reply from the authors, or
indication that the authors were notified. Conclusions in this study are
limited due to the small size, however we should consider all information in
the context of the full body of research.
The conference publication
for this analysis was self-censored by the authors, not due to any error in
the analysis, but because authors believe ivermectin "has proven to be
ineffective in clinical trials". This is incorrect,
64 studies show
statistically significant positive results for one or more outcomes
(37 prospective and
27 retrospective
studies, including 27
Randomized Controlled Trials).
Concerns have been raised
about Carvallo. There appears to be some valid concerns with
potential data issues, and this study is excluded in the exclusion analysis. There is no significant change in
results, with only a minor reduction in prophylaxis efficacy to 84% [73‑91%].
However, it is difficult to trust information from the personality reporting
the concerns. The author suggests that the study may not have happened at
all, claiming for example that the team could not have afforded the
medications without funding, and that a busy clinician would not have enough
time. However, with just basic checks, the author would know that a drug
company has confirmed donating the medications, that they confirmed
authorization for the study was received, that the main hospital for the
study requested additional supplies, and that the hospital confirmed ethics
committee approval. For additional details see O'Reilly. We also
note that the combined treatment in this study has been independently shown
to be effective, and the complementary mechanisms of action support improved
efficacy of the combination407.
For discussion of all studies see c19ivm.org. A few studies have
received special attention, with some considering them to be very strong
evidence overriding the other 104 studies. We
note limitations of these studies here.
Loading..
Loading..
Loading..
Loading..
Phone survey based RCT with low risk patients, 200 ivermectin
and 198 control, showing lower mortality, lower disease progression, lower
treatment escalation, and faster resolution of symptoms with treatment,
without reaching statistical significance. Authors find the results of this
trial alone do not support the use of ivermectin. However the effects are all
positive, especially for serious outcomes which are unable to reach
statistical significance with the very small number of events in the low risk
population.
An open letter, signed by >100 physicians, concluding this
study is fatally flawed can be found at jamaletter.com.
With the low risk patient population, there is little room for
improvement with an effective treatment - 59/57% (IVM/control) recovered
within the first 2 days to either "no symptoms" or "not hospitalized and no
limitation of activities"; 73/69% within 5 days. Less than 3% of all patients
ever deteriorated.
The primary outcome was changed mid-trial, it was originally
clinical deterioration, which is more meaningful, and shows greater benefit.
The new outcome of resolution of symptoms includes "not hospitalized and no
limitation of activities" as a negative outcome and is not very meaningful in
terms of assessing how much treatment reduces serious outcomes. Using this
measure could completely invalidate results - for example a treatment that
eliminates all COVID-19 symptoms but has a temporary minor adverse event
could be seen as worse.
Authors state that "preliminary reports of other randomized
trials of ivermectin as treatment for COVID-19 with positive results have not
yet been published in peer-reviewed journals", however there were 8
peer-reviewed RCTs with positive effects published prior to this paper(and 19
total peer-reviewed studies with positive effects).
Authors advised taking ivermectin on an empty stomach, reducing
lung tissue concentration by ~2.5x1.
76 patients were excluded due to control patients receiving
ivermectin. However, there was a similar percentage of adverse events like
diarrhea, nausea, and abdominal pain in both treatment and control groups.
These are potential non-serious side effects of treatment and suggest that it
is possible that many more control patients received some kind of
treatment.
No pre-registered protocol documentation has been found, the
same organization is associated with other COVID trials with extremely high
financial conflicts of interest with this trial, and the official registration
shows a different code to the paper (IVE-PA_CEIP vs. PI-CEP-1390)643.
Ivermectin was widely used in the population and available OTC
at the time of the study. The paper claims that patients were excluded if they
used ivermectin within the last 5 days, however this conflicts with the trial
registration which shows that use of ivermectin within the previous 2 days was
an exclusion criterion. A post-hoc change to 5 days was made on December 16,
2020644,645,
which is after enrollment ended (July 15 to November 30, 2020). Ivermectin
may retain efficacy far beyond 2 or 5 days. Note that, with 75% of patients
having symptoms for 4+ days at baseline, the trial registration allows
patients to take ivermectin for a few days after symptoms and then join the
placebo arm two days later646.
The study reports 11.5% blurry vision with ivermectin,
consistent with known side effects. However, the study also reports 11.6%
blurry vision in the placebo group, which is not consistent with expected side
effects of placebo. One possible explanation is that many placebo patients
received ivermectin.
This study reportedly has an ethical issue whereby participants
were told the study drug was "D11AX22"647.
The editor-in-chief of JAMA initially offered to help with this issue, but
later indicated that "JAMA does not review consent forms", however the lead
author reportedly confirmed the issue648-650.
The study protocol specifically allows "the use of other
treatments outside of clinical trials". The paper provides no information on
what other treatments were used, but other treatments were commonly used at
the time. Additionally, the control group did about 5x better than
anticipated for deterioration, also suggesting that the control patients used
some kind of treatment. Patients that enroll in such a study may be more
likely to learn about and use other treatments, especially since they do not
know if they are receiving the study medication.
The study protocol was amended 4 times. Amendments 2-4 are
provided but amendment 1 is missing. Amendment 2 increased the inclusion
criteria to within 7 days of onset, including more later stage patients and
reducing the expected effectiveness. The trial protocol lists “the duration
of supplemental oxygen” as an outcome but the results for this outcome are
missing.
RCTs have a fundamental bias against finding an effect for
interventions that are widely available — patients that believe they
need treatment are more likely to decline participation and take the
intervention388, i.e., RCTs are more likely to enroll low-risk
participants that do not need treatment to recover (this does not apply to
the typical pharmaceutical trial of a new drug that is otherwise
unavailable). This trial was run in a community where ivermectin was
available OTC and very widely known and used.
Grants and/or personal fees, including in some cases during the
conduct of the study, were provided by Sanofi Pasteur, GlaxoSmithKline,
Janssen, Merck, and Gilead. For more details see651.
With only 7% hospitalization, this trial is underpowered. The trial primarily
includes low-risk patients that recover quickly without treatment, leaving
minimal room for improvement with treatment. 74 patients had symptoms for >= 7
days. Among the 7 patients requiring ventilation, authors note that the
earlier requirement in the ivermectin group may be due to those patients
having higher severity at baseline. However, authors know the answer to this -
it is unclear why it is not reported. There were more adverse events in the
placebo group than the ivermectin group, suggesting a possible issue with
dispensing or non-trial medication usage. 25+% of patients were hospitalized
within 2/3 days for the placebo/treatment groups (Figure S2).
The companion prophylaxis study IVERCOR PREP has
reported results in the press and an online presentation655,656,
however these results have not yet been formally published. The prophylaxis
study results are very positive and statistically significant, and would be
expected to receive priority publication due to the predicted impact on the
pandemic and confirmation of previous prophylaxis studies. The lack of formal
publication suggests a negative publication bias that may be due to
politicization in the authors' location.
Authors pre-specify multivariate analysis but do not present
it, however multivariate analysis could significantly change the results.
Consider for example if just a few extra patients in the ivermectin group
were in severe condition based on baseline SpO2. The lower mean SpO2 in the
ivermectin group, and the shorter time to ventilation, are consistent with
this being the case. Additionally, there are 14% more male patients in the
ivermectin group.
An extremely large percentage of patients (55%) were excluded
based on ivermectin use in the last 7 days. However, ivermectin may retain
efficacy much longer (for example antiparasitic activity may persist for
months398). A significant number of patients may also
misrepresent their prior and future usage — the population is clearly
aware of ivermectin, and patients with progressing disease may be motivated
to take it, knowing that they may be in the control group. Another report
states that 12,000 patients were excluded for recent use of ivermectin657).
RCTs have a fundamental bias against finding an effect for
interventions that are widely available — patients that believe they
need treatment are more likely to decline participation and take the
intervention388, i.e., RCTs are more likely to enroll low-risk
participants that do not need treatment to recover (this does not apply to
the typical pharmaceutical trial of a new drug that is otherwise
unavailable). This trial was run in a community where ivermectin was very
widely known and used.
For other issues see
trialsitenews.com (K).
Another study reports results on a larger group of patients in
the same hospital, showing ivermectin mortality RR 0.81 [0.53-1.24]659.
Questions have been raised about this study and the early
termination of the study and discontinuation of treatments, because the
hospital statistics show a dramatically lower (~75%) case fatality rate
during the period of the study660 (data from gob.mx).
| Date | Cases | Deaths | CFR |
| 3/2020 | 2 | 1 | 50% |
| 4/2020 | 4 | 1 | 25% |
| 5/2020 | 13 | 1 | 8% |
| 6/2020 | 37 | 2 | 5% |
| 7/2020 | 65 | 5 | 8% |
| 8/2020 | 79 | 23 | 29% |
| 9/2020 | 54 | 12 | 22% |
| 10/2020 | 62 | 21 | 34% |
| 11/2020 | 80 | 26 | 33% |
| 12/2020 | 41 | 13 | 32% |
Several other inconsistencies have been reported163.
This meta analysis is designed to exclude most studies. Authors
select a small subset of studies, with a majority of results based on only 1
or 2 studies. Authors split up studies which dilutes the effects and results
in a lack of statistical significance for most outcomes. Authors perform 16+
meta analyses with very few studies in each analysis, and do not combine the
evidence from all studies. However, we can consider the probability of the
observed results across all outcomes.
Authors find positive results for 11 of 12 primary efficacy
outcomes with events, or 16 of 18 including secondary outcomes. One of the
primary outcomes and two of the secondary outcomes show statistically
significant improvements in isolation. If we assume independence, the
probability that 11+ of 12 primary efficacy outcomes were positive for an
ineffective treatment is p = 0.003. For 16+ of 18 outcomes we get
p = 0.0007. This simple analysis does not take into account the
magnitude of positive effects, or the dependence due to some studies
contributing multiple outcomes, however observation suggests that a full
analysis of the combined evidence is likely to show efficacy.
The study is entirely retrospective in the current version. The
protocol is dated April 20, 2021, and the most recent study included is from
March 9, 2021. The protocol was modified after publication in order to include
a close to null result (Beltran Gonzalez "patients discharged without
respiratory deterioration or death at 28 days"), so the current protocol is
dated July 28, 2021.
Authors excluded many studies by requiring results at a
specific time, for example mortality, ventilation, etc. required results at
exactly 28 days. Authors excluded all prophylaxis studies by requiring
results at exactly 14 days.
Studies comparing with other medications were excluded, however
these studies confirm efficacy of ivermectin. The only case where they could
overstate the efficacy of ivermectin is if the other medication was harmful.
There is some evidence of this for excessive dosage/very late stage use,
however that does not apply to any of the studies here.
Studies using combined treatment were excluded, even when it is
known that the other components have minimal or no effect. 3 of 4 RCTs with
combined treatment use doxycycline in addition, which was shown to have no
significant effect in Butler (B). Other studies were excluded by
requiring PCR confirmation.
Authors are inconsistent regarding active comparators. They
state that hydroxychloroquine “does not work”, yet excluded trials comparing
ivermectin to a drug they hold to be inactive. On the other hand, remdesivir
was an acceptable comparator, although it is considered to be effective
standard of care in some locations358.
Authors fail to recognize that Risk of Bias (RoB) domains such
as blinding are far less important for the objective outcome of
mortality.
Authors include Beltran Gonzalez as "moderate"
COVID-19, however patients in this study were in severe condition (baseline
SatO2 83).
Fordham summarizes several problems:
•unsupported assertions of adverse
reactions to ivermectin, and the outdated claim that unsafe dosing would be
needed to be effective;
•a demand for PCR or antigen testing,
without analysis of reliability and not universally available even in
developed countries at the start of the pandemic;
•contradictions in the exclusion
criteria, including placebo and approved SoC comparators, but rejecting
hydroxychloroquine, though held to be ineffective (and an approved SoC in
some jurisdictions);
•inclusion of “deemed active”
comparators whilst excluding “potentially active” ones;
•exclusion of combination therapies,
though the norm among practising clinicians;
•the rejection of other than RCTs when
the objective is a “complete evidence profile”;
•arbitrary time-points for outcome
measures, excluding non-compliant trials;
•fragmentation of data by location of
care under varying hospitalisation criteria;
•the resulting focus on a small
fraction of the available clinical evidence, with most comparisons based on
single studies with no meta-analysis possible;
•a resulting inpatient mortality
comparison with fewer patients than a June 2020 confounder-matched
study;
•no conclusion on the headline
mortality outcome, when multiple lines of evidence from elsewhere
(including the WHO) point to significant mortality advantage.
Cochrane was reputable in the past, but is now controlled by
pharmaceutical interests. For example, see the news related to the expulsion
of founder Dr. Gøtzsche and the associated mass resignation of board members
in protest664-666.
For another example of bias see ebm.bmj.com.
The BiRD group gave the following early comment: "Yesterday’s
Cochrane review surprisingly doesn’t take a pragmatic approach comparing
ivermectin versus no ivermectin, like in the majority of other existing
reviews. It uses a granular approach similar to WHO’s and the flawed Roman et
al paper, splitting studies up and thereby diluting effects. Consequently,
the uncertain conclusions add nothing to the evidence base. A further
obfuscation of the evidence on ivermectin and an example of research waste.
Funding conflicts of interests of the authors and of the journal concerned
should be examined."
For dicussion of issues added in the updated version see
Popp.
Please submit updates and
corrections at https://c19ivm.org/meta.html.
6/20/2025: PRINCIPLE trial discussion updates.
4/26/2025: Preclinical updates.
3/20/2025: Preclinical updates.
12/7: Discussion updates.
11/1: We added Bagheri-Far.
7/22: We added Wijewickrema.
6/13: We added Hashmi.
5/3: We added Varnaseri.
3/30: Updated discussion of pooled outcomes.
3/29: We added Siripongboonsitti.
3/9: Discussion updates.
2/29: We added Hayward.
2/23: RCT discussion updates.
2/12: We added Oranu.
1/24/2024: We updated the introduction.
12/27: We added Mikamo.
9/23: Preclinical updates.
8/10: Preclinical updates.
7/25: We added Osati.
7/17: We updated the introduction.
6/11: We added Llenas-García.
6/6: We added Wada.
4/21: We added Munir.
4/18: We updated Desort-Henin to the published version.
2/23: We updated Schilling to the journal version.
1/6/2023: We added Desort-Henin, Sarojvisut.
12/20: We updated the discussion of heterogeneity and
RCTs.
12/15: We added the ACTIV-6 600µg/kg arm
Naggie (B).
12/9: We updated de la Rocha to the journal version.
10/27: We added Ochoa-Jaramillo.
10/21: We updated the ACTIV-6 trial to the journal version.
9/23: We added Aref (B).
9/9: We added Qadeer.
8/18: We added Bramante.
7/26: We added Schilling.
6/24: We added Mirahmadizadeh.
6/16: We updated the ACTIV-6 analysis.
6/12: We added Naggie.
6/1: We updated the Together Trial analysis.
5/30: We added George.
5/30: We updated the Together Trial analysis.
5/27: We added de la Rocha.
4/25: SSC discussion updates.
4/17: We added a section on preclinical research.
4/16: We added discussion of the NIH recommendation.
4/9: We updated the Together Trial analysis.
4/8: We added Ravikirti.
4/5: We added preprint discussion based on Zeraatkar, and updated the Together Trial analysis.
4/2: We updated the Together Trial analysis.
3/30: We updated Reis to the journal version.
3/21: Strongyloides discussion updates.
3/3: We updated Beltran Gonzalez to the journal version.
3/2: We added Soto.
2/28: We added Efimenko.
2/25: We added Thairu.
2/23: We updated Mayer to the journal version.
2/18: We updated Lim to the journal version.
2/2: We added Manomaipiboon.
1/28: We added de Jesús Ascencio-Montiel.
1/21: We added Zubair.
1/17: We added an explanation of why funnel plot analysis is not valid in this case.
1/16: We added RCT viral clearance analysis and corrected
missing symptomatic case results in the case analysis.
1/15: We updated Kerr to the journal version.
1/15: We corrected hospitalization group sizes in Buonfrate.
1/11: We updated Kerr to the latest results, and
added discussion of Beltran Gonzalez.
12/31: We added Shimizu.
12/29: We added Mustafa.
12/26: We updated Kerr to the revised version of the
paper.
12/16: We added Jamir.
12/11: We added Kerr.
12/8: We added analysis of the number of independent research
groups reporting statistically significant positive results.
12/5: We added Ferreira.
12/5: We added Rezk.
12/3: A note on Bernigaud: continuity correction uses the
reciprocal of the contrasting arm Sweeting, as detailed in the
appendix. We previously limited the size of the control group when showing the
total number of patients, however this was confusing for people that did not
read the details, as discussed below. The full group size has always been used
when computing the RR.
12/1: Strongyloides
discussion updates.
11/30: We corrected Ghauri to use the event
counts.
11/24: We added Ozer.
11/24: SSC
discussion updates.
11/21: Strongyloides
discussion updates.
11/20: Strongyloides
discussion updates.
11/19: We added analysis by strongyloides prevalence, and updated it to match
the revised classification used in the comparable analysis.
11/19: We added additional exclusion analyses in the
supplementary data.
11/18: We incorrectly included López-Medina as a study
not reporting use of steroids, however they report 6% usage in the control
group.
11/18: We added Samajdar.
11/17: SSC response.
11/16: Discussion updates.
11/12: We now show the number of studies reporting
statistically significant results for any outcome, primary outcomes, and the
most serious outcome.
11/9: Discussion updates.
11/5: We added discussion of strongyloides, comparison with the recent molnupiravir approval, and notes on recruitment for remote outpatient delayed treatment
trials.
11/3: We added Lim.
11/3: Discussion updates.
10/29: Discussion updates including GMK vitamin D analysis.
10/28: Discussion updates.
10/26: We updated the GMK
response.
10/24: We added additional exclusion analyses for individual
outcomes.
10/21: We added Borody.
10/19: Discussion updates.
10/18: Ghauri was updated to the journal version.
10/16: We added a summary plot for all results.
10/13: We added primary outcome analysis and additional
exclusion analyses. Niaee et al. has been reported as pending retraction and
has been removed. 10/27 update: the journal has reported that this is
incorrect — no retraction is pending.
10/11: Discussion updates. Niaee et al. exclusion. Updates to
the study notes including discussion of
Vallejos et al. and additional issues in
the Together Trial. Discussion of inherent bias in RCTs for widely available
interventions.
10/8: Discussion updates.
10/7: Samaha et al. has been reported as pending retraction and
has been removed. There was no significant change in the results.
10/4: Merck discussion updates.
9/29: We corrected a display error causing a few points to be missing in Figure 4.
9/27: We added Mayer.
9/24: We added a graph of variants over time for the Together
Trial discussion and corrected outcome discussion for Popp et al.
9/22: Discussion updates.
9/20: Discussion updates.
9/18: We added Buonfrate, and updated discussion of
the Together Trial.
9/17: We added study notes.
9/15: Discussion updates.
9/14: FDA discussion updates.
9/9: We added sensitivity analysis to compute the minimum
number of studies that need to be excluded in order to avoid showing
efficacy. Discussion updates.
9/7: Discussion updates.
9/6: We corrected Espitia-Hernandez to use the
reported recovery time and added missing recovery and viral clearance
results.
9/3: We updated discussion and excluded Carvallo et al. in the
exclusion analysis.
8/27: We updated Morgenstern (B) with the journal version
of the article.
8/26: We updated Mohan with the journal version of
the article.
8/16: We updated Reis with event
counts.
8/15: We updated discussion and made the abstract more
concise.
8/8: We updated discussion in the responses.
8/6: We updated Behera (B) with the journal version
of the article.
8/5: We added Mondal.
8/4: We added discussion of the FDA recommendation.
8/3: We added discussion in the responses section.
8/2: We added analysis restricted to serious outcomes and
analysis restricted to recovery, and we added discussion in the responses section.
7/31: We added discussion in the responses section related to in vitro evidence
and therapeutic concentrations.
7/29: We added discussion in the responses section.
7/20: We updated Hashim with the journal version
of the article.
7/16: We updated Ravikirti (B) with the journal version
of the article.
7/15: Elgazzar et al. was withdrawn by the preprint server and
has been removed.
7/9: We added Hazan (B).
7/8: We updated Cadegiani to the journal version.
7/6: We previously limited the size of the control group for
Bernigaud when calculating the total number of patients, however
this was confusing for many people that did not read the details. We now
show the original counts and note the larger size of the control group in the
text.
7/3: We added Vallejos.
7/2: We updated Niaee et al. to the journal version.
6/21: We added more information to the abstract.
6/19: We updated Bryant to the journal version.
6/19: Beltran Gonzalez was incorrectly included in the peer-reviewed analysis.
6/18: We added Krolewiecki.
6/15: We added Aref.
6/7: We added Hariyanto.
6/5: We added Ahsan.
6/2: We added Abd-Elsalam.
5/31: Biber was updated to the preprint.
5/26: Samaha et al. was updated to the journal version.
5/18: We added analysis of Merck's recommendation.
5/17: We added Szente Fonseca.
5/15: We updated the discussion of the WHO analysis.
5/13: We updated Mahmud to the journal version.
5/10: We added Faisal.
5/10: We added additional information in the abstract.
5/8: We added Merino.
5/7: We updated Shahbaznejad to the journal version,
which includes additional outcomes not reported earlier.
5/6: We updated Chahla to the Research Square preprint.
5/6: We added a comparison of CDC recommendations.
5/6: We added mechanical ventilation and ICU admission
analysis.
5/6: We updated discussion based on peer review including
discussion of heterogeneity, exclusion based sensitivity analysis, and search
criteria.
5/5: We updated Okumuş to the journal paper.
5/5: We previously limited the size of the control group in
Bernigaud to be the same as the treatment group for calculation of
the total number of patients. This is now also reflected and noted in the
forest plots.
5/4: We added Loue.
4/30: We added analysis of the WHO meta analysis and updated
Kory to the journal version.
4/28: We added the WHO meta analysis results for
comparison.
4/27: We added analysis restricted to hospitalization results
and a comparison with the evidence base used in the approval of other
COVID-19 treatments.
4/26: We added notes on heterogeneity.
4/25: We updated Biber to the latest results reported at the International Ivermectin for Covid Conference.
4/18: We updated Morgenstern to the preprint.
4/16: We added Morgenstern.
4/14: We added Seet.
4/10: We added Kishoria.
4/9: We corrected a duplicate entry for
Bukhari.
4/7: We identified studies where minimal detail is currently
available in the forest plots.
4/5: We added Mourya.
4/4: We added event counts to the forest plots.
3/31: We updated Chahla (B) to the preprint.
3/30: We added Chahla.
3/28: We highlighted and added discussion for studies that use
combined treatments.
3/26: We added Tanioka.
3/25: We added Huvemek.
3/17: We added Nardelli.
3/10: We added Pott-Junior.
3/6: We added Chowdhury and we identify studies that
compare with another treatment.
3/5: We added discussion of pooled effects (we show both pooled
effects and individual outcome results).
3/4: We added López-Medina, and we added more information in the abstract.
3/3: We updated the graphs to indicate the time period for the
dosage column, now showing the dosage over one month for prophylaxis and over
four days for other studies.
3/2: We updated IVERCOR PREP with the latest results
Vallejos (B).
2/27: We added analysis restricted to peer reviewed
studies.
2/24: We added a comparison of the evidence base and WHO
approval status for the use of ivermectin with scabies and COVID-19. We
updated Okumuş with the Research Square preprint.
2/23: We added Beltran Gonzalez.
2/18: We updated Babalola to the journal version of
the paper.
2/17: We added Elalfy, and we added analysis
restricted to viral clearance outcomes, and mortality results restricted to
RCTs.
2/16: We updated Behera to the journal version of
the paper.
2/15: We added Behera (B).
2/14: We added analysis restricted to COVID-19 case outcomes,
and we added additional results in the abstract.
2/12: We added Biber.
2/11: We added more details on the analysis of prospective vs.
retrospective studies.
2/10: We added Lima-Morales.
2/5: We updated Bukhari to the preprint.
2/2: We added Mohan.
1/26: We updated Shouman (B) with the journal version of
the article.
1/25: We updated IVERCOR PREP with the recently released
results.
1/19: We added Shahbaznejad and Samaha et al. Chaccour (B) was
updated to the journal version of the paper.
1/17: We added Bukhari.
1/16: We moved the analysis with exclusions to the main text,
and added additional commentary.
1/15: We added the effect measured for each study in the forest
plots.
1/12: We added Okumuş.
1/11: We added Chahla (B).
1/10: We put all prophylaxis studies in a single group.
1/9: We added Ravikirti (B). Due to the much larger size of
the control group in Bernigaud, we limited the size of the control
group to be the same as the treatment group for calculation of the total
number of patients.
1/7: We added direct links to the study details in the
chronological plots.
1/6: We added Babalola.
1/5: We added direct links to the study details in the forest
plots.
1/2/2021: We added dosage information and we added the number of
patients to the forest plots.
12/31: We added additional details about the studies in the
appendix.
12/29: We added meta analysis excluding late treatment.
12/27: We added the total number of authors and patients.
12/26: We added IVERCOR PREP, Carvallo (B).
12/17: We added Alam.
12/16: We added Ghauri.
12/11: We added Soto-Becerra.
12/7: We added Chaccour (B).
12/2: We added Ahmed.
11/26/2020: Initial revision.
We perform ongoing searches of PubMed, medRxiv, Europe PMC,
ClinicalTrials.gov, The Cochrane Library, Google Scholar, Research
Square, ScienceDirect, Oxford University Press, the reference lists of other
studies and meta-analyses, and submissions to the site c19ivm.org, which regularly receives submissions of studies upon publication.
Search terms are ivermectin and COVID-19 or SARS-CoV-2. Automated searches are performed twice daily, with all matches reviewed for inclusion.
All studies regarding the use of ivermectin for COVID-19 that report
a comparison with a control group are included in the main analysis.
Sensitivity analysis is performed, excluding studies with major issues,
epidemiological studies, and studies with minimal available information.
Studies with major unexplained data issues, for example major outcome data that
is impossible to be correct with no response from the authors, are excluded.
However for ivermectin certain high-profile studies that would normally be
retracted currently remain published due to the politicization of this treatment—for
transparency, and because inclusion does not affect the results, we currently include these
studies.
This is a living analysis and is updated regularly.
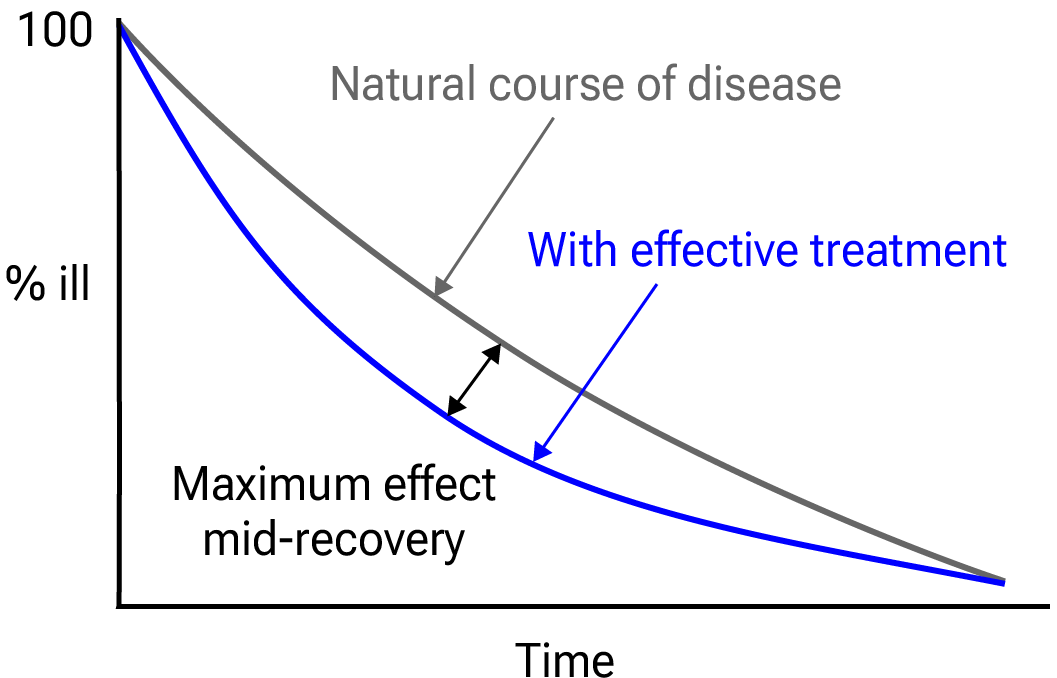{kind=link}

Figure 36.
Mid-recovery results can more accurately reflect efficacy when almost all patients
recover. Mateja et al. confirm that intermediate viral load results more accurately
reflect hospitalization/death.
We extracted effect sizes and associated data from all studies.
If studies report multiple kinds of effects then the most serious
outcome is used in pooled analysis, while other outcomes are included in the
outcome specific analyses. For example, if effects for mortality and cases are
reported then they are both used in specific outcome analyses, while mortality
is used for pooled analysis.
If symptomatic
results are reported at multiple times, we use the latest time, for example
if mortality results are provided at 14 days and 28 days, the results at 28
days have preference. Mortality alone is preferred over combined outcomes.
Outcomes with zero events in both arms are not used, the next most serious
outcome with one or more events is used. For example, in low-risk populations
with no mortality, a reduction in mortality with treatment is not possible,
however a reduction in hospitalization, for example, is still valuable.
Clinical outcomes are considered more important than viral outcomes.
When basically all patients recover in both treatment and control groups,
preference for viral clearance and recovery is given to results mid-recovery
where available. After most or all patients have recovered there is little or
no room for an effective treatment to do better, however faster recovery is
valuable.
An IPD meta-analysis confirms that intermediate viral load reduction
is more closely associated with hospitalization/death than later
viral load reduction682.
If only individual symptom data is available, the most serious symptom has
priority, for example difficulty breathing or low SpO2 is more
important than cough.
When results provide an odds ratio, we compute the relative risk when
possible, or convert to a relative risk according to Zhang (C) et al.
Reported confidence intervals and p-values are used when available,
and adjusted values are used when provided. If multiple types of adjustments are
reported propensity score matching and multivariable regression has preference
over propensity score matching or weighting, which has preference over
multivariable regression. Adjusted results have preference over unadjusted
results for a more serious outcome when the adjustments significantly alter
results. When needed, conversion between reported p-values and
confidence intervals followed Altman, Altman (B), and Fisher's exact
test was used to calculate p-values for event data. If continuity
correction for zero values is required, we use the reciprocal of the opposite
arm with the sum of the correction factors equal to 1678.
Results are expressed with RR < 1.0 favoring treatment, and using the risk of
a negative outcome when applicable (for example, the risk of death rather than
the risk of survival). If studies only report relative continuous values such
as relative times, the ratio of the time for the treatment group versus the
time for the control group is used. Calculations are done in Python
(3.13.5) with
scipy (1.16.0), pythonmeta (1.26), numpy (2.3.1), statsmodels (0.14.4), and plotly (6.2.0).
Forest plots are computed using PythonMeta686
with the DerSimonian and Laird random effects model (the fixed effect
assumption is not plausible in this case) and inverse variance weighting.
Results are presented with 95% confidence intervals. Heterogeneity among studies was
assessed using the I2 statistic.
Mixed-effects meta-regression results are computed with R (4.4.0) using the metafor
(4.6-0) and rms (6.8-0) packages, and using the most serious sufficiently powered outcome.
Forest plots show simplified dosages for comparison, these are the total dose in the first four days for treatment, and the monthly dose for prophylaxis, for a 70kg person. For full dosage details see below.
For all statistical tests, a p-value less than 0.05 was considered statistically significant.
Grobid 0.8.2 is used to parse PDF documents.
We have classified studies as early treatment if most patients
are not already at a severe stage at the time of treatment (for example based
on oxygen status or lung involvement), and treatment started within 5 days of
the onset of symptoms. If studies contain a mix of early treatment and late
treatment patients, we consider the treatment time of patients contributing
most to the events (for example, consider a study where most patients are
treated early but late treatment patients are included, and all mortality
events were observed with late treatment patients).
We note that a shorter time may be preferable. Antivirals are typically only
considered effective when used within a shorter timeframe, for example 0-36 or
0-48 hours for oseltamivir, with longer delays not being effective190,191.
We received no funding, this research is done in our spare
time. We have no affiliations with any pharmaceutical companies or political
parties.
Note that the size of the control group in Bernigaud
is significantly larger than the treatment group. We previously limited the
size to be the same as that of the treatment group for calculation of the
number of patients, however this was confusing to many people that did not
read the details.
A summary of study results is below. Please submit
updates and corrections at https://c19ivm.org/meta.html.
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| Abbas, 12/31/2021, Double Blind Randomized Controlled Trial, placebo-controlled, China, peer-reviewed, 3 authors, study period May 2021 - August 2021, dosage 300μg/kg days 1-5, excluded in exclusion analyses: very minimal patient information, three different results for the recovery outcome, selective omission of the statistically significant recovery p-value, and other inconsistencies. | risk of death, 4.0% higher, RR 1.04, p = 1.00, treatment 1 of 99 (1.0%), control 1 of 103 (1.0%). |
| deterioration of 2 or more points, 40.5% lower, RR 0.59, p = 0.54, treatment 4 of 99 (4.0%), control 7 of 103 (6.8%), NNT 36. | |
| escalation of care, 14.9% lower, RR 0.85, p = 0.82, treatment 9 of 99 (9.1%), control 11 of 103 (10.7%), NNT 63. | |
| fever during study, 17.9% lower, RR 0.82, p = 0.58, treatment 15 of 99 (15.2%), control 19 of 103 (18.4%), NNT 30. | |
| risk of no recovery, 35.6% lower, RR 0.64, p = 0.04, treatment 26 of 99 (26.3%), control 42 of 103 (40.8%), NNT 6.9, primary outcome. | |
| recovery time, 30.8% lower, relative time 0.69, p = 0.08, treatment 99, control 103, primary outcome. | |
| Ahmed, 12/2/2020, Double Blind Randomized Controlled Trial, Bangladesh, peer-reviewed, mean age 42.0, 15 authors, average treatment delay 3.83 days, dosage 12mg days 1-5, the ivermectin + doxycycline group took only a single dose of ivermectin. | risk of unresolved symptoms, 85.0% lower, RR 0.15, p = 0.09, treatment 0 of 17 (0.0%), control 3 of 19 (15.8%), NNT 6.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 7, fever, ivermectin (5 days), primary outcome. |
| risk of unresolved symptoms, 62.7% lower, RR 0.37, p = 0.35, treatment 1 of 17 (5.9%), control 3 of 19 (15.8%), NNT 10, day 7, fever, ivermectin (1 day) + doxycycline. | |
| risk of no viral clearance, 75.6% lower, HR 0.24, p = 0.03, treatment 11 of 22 (50.0%), control 20 of 23 (87.0%), NNT 2.7, adjusted per study, inverted to make HR<1 favor treatment, day 7, ivermectin (5 days). | |
| risk of no viral clearance, 56.5% lower, HR 0.43, p = 0.22, treatment 16 of 23 (69.6%), control 20 of 23 (87.0%), NNT 5.8, adjusted per study, inverted to make HR<1 favor treatment, day 7, ivermectin (1 day) + doxycycline. | |
| risk of no viral clearance, 63.0% lower, HR 0.37, p = 0.02, treatment 5 of 22 (22.7%), control 14 of 23 (60.9%), NNT 2.6, adjusted per study, inverted to make HR<1 favor treatment, day 14, ivermectin (5 days). | |
| risk of no viral clearance, 41.2% lower, HR 0.59, p = 0.19, treatment 9 of 23 (39.1%), control 14 of 23 (60.9%), NNT 4.6, adjusted per study, inverted to make HR<1 favor treatment, day 14, ivermectin (1 day) + doxycycline. | |
| time to viral-, 23.6% lower, relative time 0.76, p = 0.02, treatment 22, control 23, ivermectin (5 days). | |
| time to viral-, 9.4% lower, relative time 0.91, p = 0.27, treatment 23, control 23, ivermectin (1 day) + doxycycline. | |
| Aref, 6/15/2021, Randomized Controlled Trial, Egypt, peer-reviewed, 7 authors, study period February 2021 - March 2021, dosage not specified, trial NCT04716569 (history). | relative duration of fever, 63.2% lower, relative time 0.37, p < 0.001, treatment 57, control 57, primary outcome. |
| relative duration of dyspnea, 56.4% lower, relative time 0.44, p < 0.001, treatment 57, control 57. | |
| relative duration of anosmia, 68.8% lower, relative time 0.31, p < 0.001, treatment 57, control 57. | |
| relative duration of cough, 64.3% lower, relative time 0.36, p < 0.001, treatment 57, control 57. | |
| risk of no viral clearance, 78.6% lower, RR 0.21, p = 0.004, treatment 3 of 57 (5.3%), control 14 of 57 (24.6%), NNT 5.2. | |
| time to viral-, 35.7% lower, relative time 0.64, p < 0.001, treatment 57, control 57. | |
| Babalola, 1/6/2021, Double Blind Randomized Controlled Trial, Nigeria, peer-reviewed, baseline oxygen required 8.3%, 10 authors, study period May 2020 - November 2020, dosage 12mg or 6mg q84h for two weeks, this trial compares with another treatment - results may be better when compared to placebo. | adjusted risk of viral+ at day 5, 63.9% lower, RR 0.36, p = 0.11, treatment 40, control 20, adjusted per study, inverted to make RR<1 favor treatment. |
| relative ∆SpO2 (unadjusted), 41.5% better, RR 0.59, p = 0.07, treatment 38, control 18, figure 3. | |
| risk of no viral clearance, 58.0% lower, HR 0.42, p = 0.01, treatment 20, control 20, inverted to make HR<1 favor treatment, 12mg - Cox proportional hazard model. | |
| risk of no viral clearance, 40.5% lower, HR 0.60, p = 0.12, treatment 20, control 20, inverted to make HR<1 favor treatment, 6mg - Cox proportional hazard model. | |
| time to viral-, 49.2% lower, relative time 0.51, p = 0.02, treatment 20, control 20, 12mg, primary outcome. | |
| time to viral-, 34.4% lower, relative time 0.66, p = 0.08, treatment 20, control 20, 6mg. | |
| Biber, 2/12/2021, Double Blind Randomized Controlled Trial, placebo-controlled, Israel, peer-reviewed, 10 authors, study period 12 May, 2020 - 31 October, 2020, average treatment delay 4.0 days, dosage 12mg days 1-3, 15mg for patients ≥70kg, trial NCT04429711 (history). | risk of hospitalization, 70.2% lower, RR 0.30, p = 0.34, treatment 1 of 47 (2.1%), control 3 of 42 (7.1%), NNT 20. |
| risk of no viral clearance, 61.6% lower, RR 0.38, p = 0.02, treatment 8 of 47 (17.0%), control 17 of 42 (40.5%), NNT 4.3, adjusted per study, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, Ct>30, multivariable, day 8. | |
| risk of no viral clearance, 39.0% lower, RR 0.61, p = 0.09, treatment 13 of 47 (27.7%), control 21 of 42 (50.0%), NNT 4.5, adjusted per study, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, Ct>30, multivariable, day 6, primary outcome. | |
| risk of no viral clearance, 73.0% lower, RR 0.27, p = 0.008, treatment 3 of 23 (13.0%), control 14 of 29 (48.3%), NNT 2.8, culture viability. | |
| risk of no viral clearance, 70.2% lower, RR 0.30, p = 0.14, treatment 2 of 47 (4.3%), control 6 of 42 (14.3%), NNT 10.0, non-infectious samples (Ct>30 or non-viable culture), day 10. | |
| risk of no viral clearance, 82.1% lower, RR 0.18, p = 0.01, treatment 2 of 47 (4.3%), control 10 of 42 (23.8%), NNT 5.1, non-infectious samples (Ct>30 or non-viable culture), day 8. | |
| risk of no viral clearance, 75.6% lower, RR 0.24, p = 0.02, treatment 3 of 47 (6.4%), control 11 of 42 (26.2%), NNT 5.0, non-infectious samples (Ct>30 or non-viable culture), day 6. | |
| risk of no viral clearance, 65.1% lower, RR 0.35, p = 0.05, treatment 4 of 28 (14.3%), control 9 of 22 (40.9%), NNT 3.8, non-infectious samples (Ct>30 or non-viable culture), day 4. | |
| risk of no viral clearance, 51.9% lower, RR 0.48, p = 0.08, treatment 7 of 47 (14.9%), control 13 of 42 (31.0%), NNT 6.2, Ct>30, day 10. | |
| risk of no viral clearance, 57.9% lower, RR 0.42, p = 0.02, treatment 8 of 47 (17.0%), control 17 of 42 (40.5%), NNT 4.3, Ct>30, day 8. | |
| risk of no viral clearance, 44.7% lower, RR 0.55, p = 0.049, treatment 13 of 47 (27.7%), control 21 of 42 (50.0%), NNT 4.5, Ct>30, day 6. | |
| risk of no viral clearance, 31.9% lower, RR 0.68, p = 0.16, treatment 13 of 28 (46.4%), control 15 of 22 (68.2%), NNT 4.6, Ct>30, day 4. | |
| Borody, 10/19/2021, retrospective, Australia, preprint, 2 authors, study period 1 June, 2021 - 30 September, 2021, dosage 24mg days 1-10, this trial uses multiple treatments in the treatment arm (combined with zinc and doxycycline) - results of individual treatments may vary, excluded in exclusion analyses: preliminary report with minimal details. | risk of death, 92.3% lower, RR 0.08, p = 0.03, treatment 0 of 600 (0.0%), control 6 of 600 (1.0%), NNT 100, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of hospitalization, 92.9% lower, RR 0.07, p < 0.001, treatment 5 of 600 (0.8%), control 70 of 600 (11.7%), NNT 9.2, primary outcome. | |
| Bramante, 8/18/2022, Double Blind Randomized Controlled Trial, placebo-controlled, USA, peer-reviewed, 37 authors, average treatment delay 4.6 days, dosage 430μg/kg days 1-3, this trial compares with another treatment - results may be better when compared to placebo, trial NCT04510194 (history) (COVID-OUT). | risk of death, 197.1% higher, RR 2.97, p = 1.00, treatment 1 of 408 (0.2%), control 0 of 396 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), day 28. |
| risk of death/hospitalization, 26.7% lower, RR 0.73, p = 0.66, treatment 4 of 406 (1.0%), control 5 of 394 (1.3%), NNT 352, odds ratio converted to relative risk. | |
| risk of progression, 36.8% higher, RR 1.37, p = 0.33, treatment 23 of 406 (5.7%), control 16 of 394 (4.1%), odds ratio converted to relative risk, combined ER, hospitalization, death. | |
| risk of progression, 3.7% higher, RR 1.04, p = 0.78, treatment 105 of 407 (25.8%), control 96 of 391 (24.6%), odds ratio converted to relative risk, combined hypoxemia, ER, hospitalization, death, primary outcome. | |
| risk of hospitalization, 60.8% lower, RR 0.39, p = 0.28, treatment 2 of 206 (1.0%), control 5 of 202 (2.5%), NNT 66, IVM vs. placebo. | |
| risk of hospitalization, 74.6% lower, RR 0.25, p = 0.37, treatment 1 of 137 (0.7%), control 4 of 139 (2.9%), NNT 47, IVM vs. placebo, ≤5 days from onset. | |
| risk of hospitalization, 70.1% lower, RR 0.30, p = 0.12, treatment 3 of 406 (0.7%), control 5 of 202 (2.5%), NNT 58, IVM and IVM+MF vs. placebo. | |
| risk of hospitalization, 41.8% lower, RR 0.58, p = 0.50, treatment 3 of 406 (0.7%), control 5 of 394 (1.3%), NNT 189, IVM and IVM+MF vs. placebo and MF. | |
| Bukhari, 1/16/2021, Randomized Controlled Trial, Pakistan, preprint, 10 authors, study period 15 March, 2020 - 15 June, 2020, dosage 12mg single dose, trial NCT04392713 (history). | risk of no viral clearance, 82.4% lower, RR 0.18, p < 0.001, treatment 4 of 41 (9.8%), control 25 of 45 (55.6%), NNT 2.2, day 7, primary outcome. |
| risk of no viral clearance, 38.7% lower, RR 0.61, p < 0.001, treatment 24 of 41 (58.5%), control 43 of 45 (95.6%), NNT 2.7, day 3. | |
| Buonfrate, 9/6/2021, Double Blind Randomized Controlled Trial, Italy, peer-reviewed, 18 authors, study period 31 July, 2020 - 8 June, 2021, average treatment delay 4.0 days, dosage 1200μg/kg days 1-5, arm B 600µg/kg, arm C 1200µg/kg, trial NCT04438850 (history) (COVER), excluded in exclusion analyses: significant unadjusted group differences, with 3 times as many patients in the ivermectin arms having the baseline visit in a hospital setting, and arm C having large differences in baseline gender, weight, cough, pyrexia, and anosmia, excessive dose for arm C. | risk of hospitalization, 210.7% higher, RR 3.11, p = 0.47, treatment 1 of 28 (3.6%), control 0 of 31 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), arm B. |
| risk of hospitalization, 610.0% higher, RR 7.10, p = 0.11, treatment 3 of 30 (10.0%), control 0 of 31 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), arm C, very high dose, poorly tolerated with low compliance. | |
| relative change in viral load, RR 0.80, p = 0.59, treatment mean 2.5 (±2.2) n=28, control mean 2.0 (±4.4) n=29, day 7, arm B, primary outcome. | |
| relative change in viral load, RR 0.69, p = 0.07, treatment mean 2.9 (±1.6) n=30, control mean 2.0 (±2.1) n=29, day 7, arm C, primary outcome. | |
| Cadegiani, 11/4/2020, prospective, Brazil, peer-reviewed, 4 authors, average treatment delay 2.9 days, dosage 200μg/kg days 1-3, this trial uses multiple treatments in the treatment arm (combined with AZ, nitazoxanide (82), HCQ (22), spironolactone (66), dutasteride (4)) - results of individual treatments may vary, excluded in exclusion analyses: control group retrospectively obtained from untreated patients in the same population. | risk of death, 78.3% lower, RR 0.22, p = 0.50, treatment 0 of 110 (0.0%), control 2 of 137 (1.5%), NNT 68, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), control group 1. |
| risk of mechanical ventilation, 94.2% lower, RR 0.06, p = 0.005, treatment 0 of 110 (0.0%), control 9 of 137 (6.6%), NNT 15, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), control group 1. | |
| risk of hospitalization, 98.0% lower, RR 0.02, p < 0.001, treatment 0 of 110 (0.0%), control 27 of 137 (19.7%), NNT 5.1, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), control group 1. | |
| Carvallo (C), 9/15/2020, prospective, Argentina, peer-reviewed, mean age 55.7, 3 authors, dosage 36mg days 1, 8, dose varied depending on patient condition - mild 24mg, moderate 36mg, severe 48mg, this trial uses multiple treatments in the treatment arm (combined with dexamethasone, enoxaparin, and aspirin) - results of individual treatments may vary, excluded in exclusion analyses: minimal details of groups provided. | risk of death, 85.4% lower, RR 0.15, p = 0.08, treatment 1 of 32 (3.1%), control 3 of 14 (21.4%), NNT 5.5, moderate/severe patients, the only treatment death was a patient already in the ICU before treatment, primary outcome. |
| Chaccour (B), 12/7/2020, Double Blind Randomized Controlled Trial, Spain, peer-reviewed, 24 authors, study period 31 July, 2020 - 11 September, 2020, average treatment delay 1.0 days, dosage 400μg/kg single dose, trial NCT04390022 (history) (SAINT). | risk of symptoms, 96.0% lower, OR 0.04, p < 0.05, treatment 12, control 12, logistic regression, chance of presenting any symptom, RR approximated with OR. |
| viral load, 94.6% lower, relative load 0.05, p < 0.01, treatment 12, control 12, day 7 mid-recovery, average of gene E and gene N, data in supplementary appendix. | |
| risk of no viral clearance, 8.0% lower, RR 0.92, p = 1.00, treatment 12, control 12, primary outcome. | |
| Chahla, 3/30/2021, Cluster Randomized Controlled Trial, Argentina, peer-reviewed, 9 authors, study period September 2020 - January 2021, dosage 24mg days 1, 8, 15, 22, trial NCT04784481 (history). | risk of no discharge, 86.9% lower, RR 0.13, p = 0.004, treatment 2 of 110 (1.8%), control 20 of 144 (13.9%), NNT 8.3, adjusted per study, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, logistic regression, multivariable, primary outcome. |
| Chowdhury, 7/14/2020, Randomized Controlled Trial, Bangladesh, peer-reviewed, 6 authors, study period 2 May, 2020 - 5 June, 2020, dosage 200μg/kg single dose, this trial compares with another treatment - results may be better when compared to placebo, this trial uses multiple treatments in the treatment arm (combined with doxycycline) - results of individual treatments may vary, trial NCT04434144 (history). | risk of hospitalization, 80.6% lower, RR 0.19, p = 0.23, treatment 0 of 60 (0.0%), control 2 of 56 (3.6%), NNT 28, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of no recovery, 46.4% lower, RR 0.54, p < 0.001, treatment 27 of 60 (45.0%), control 47 of 56 (83.9%), NNT 2.6, mid-recovery day 5. | |
| recovery time, 15.2% lower, relative time 0.85, p = 0.07, treatment 60, control 56. | |
| risk of no viral clearance, 80.6% lower, RR 0.19, p = 0.23, treatment 0 of 60 (0.0%), control 2 of 56 (3.6%), NNT 28, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), primary outcome. | |
| time to viral-, 4.3% lower, relative time 0.96, p = 0.23, treatment 60, control 56. | |
| de Jesús Ascencio-Montiel, 1/24/2022, retrospective, Mexico, peer-reviewed, 10 authors, dosage 6mg days 1-2, this trial uses multiple treatments in the treatment arm (combined with AZ, acetaminophen, aspirin) - results of individual treatments may vary. | risk of death/hospitalization, 59.0% lower, RR 0.41, p < 0.001, treatment 7,898, control 20,150, adjusted per study, multivariable, primary outcome. |
| risk of death/hospitalization, 71.0% lower, RR 0.29, p < 0.001, treatment 5,557, control 12,526, adjusted per study, with phone call followup, multivariable. | |
| risk of death, 15.0% lower, RR 0.85, p = 0.16, treatment 101 of 7,898 (1.3%), control 303 of 20,150 (1.5%), NNT 445, unadjusted, excluded in exclusion analyses: unadjusted results with alternate outcome adjusted results showing significant changes with adjustments. | |
| risk of mechanical ventilation, 9.1% lower, RR 0.91, p = 0.51, treatment 77 of 7,898 (1.0%), control 216 of 20,150 (1.1%), NNT 1031, unadjusted, excluded in exclusion analyses: unadjusted results with alternate outcome adjusted results showing significant changes with adjustments. | |
| risk of hospitalization, 47.6% lower, RR 0.52, p < 0.001, treatment 485 of 7,898 (6.1%), control 2,360 of 20,150 (11.7%), NNT 18, unadjusted, excluded in exclusion analyses: unadjusted results with alternate outcome adjusted results showing significant changes with adjustments. | |
| risk of progression, 41.8% lower, RR 0.58, p < 0.001, treatment 435 of 7,898 (5.5%), control 1,906 of 20,150 (9.5%), NNT 25, unadjusted, ER, excluded in exclusion analyses: unadjusted results with alternate outcome adjusted results showing significant changes with adjustments. | |
| de la Rocha, 5/23/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Mexico, peer-reviewed, 21 authors, study period 1 July, 2020 - 29 January, 2021, dosage 12mg days 1-3, trial NCT04407507 (history), excluded in exclusion analyses: data mismatch, no response from authors. | risk of progression to serious adverse events, 186.7% higher, RR 2.87, p = 1.00, treatment 1 of 30 (3.3%), control 0 of 26 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm). |
| viral load, 2.4% lower, relative load 0.98, p = 0.64, treatment mean 33.74 (±4.77) n=30, control mean 32.94 (±7.74) n=26, day 14. | |
| viral load, 7.8% lower, relative load 0.92, p = 0.04, treatment mean 30.64 (±3.74) n=30, control mean 28.25 (±4.21) n=26, mid-recovery, day 5. | |
| Elalfy, 2/16/2021, retrospective, Egypt, peer-reviewed, 15 authors, dosage 18mg days 1, 4, 7, 10, 13, <90kg 18mg, 90-120kg 24mg, >120kg 30mg, this trial uses multiple treatments in the treatment arm (combined with nitazoxanide, ribavirin, and zinc) - results of individual treatments may vary. | risk of no viral clearance, 86.9% lower, RR 0.13, p < 0.001, treatment 7 of 62 (11.3%), control 44 of 51 (86.3%), NNT 1.3, day 15, primary outcome. |
| risk of no viral clearance, 58.1% lower, RR 0.42, p < 0.001, treatment 26 of 62 (41.9%), control 51 of 51 (100.0%), NNT 1.7, day 7. | |
| Espitia-Hernandez, 8/15/2020, retrospective, Mexico, peer-reviewed, mean age 45.1, 5 authors, dosage 6mg days 1-2, 8-9, this trial uses multiple treatments in the treatment arm (combined with azithromycin and cholecalciferol) - results of individual treatments may vary. | recovery time, 70.0% lower, relative time 0.30, p < 0.001, treatment 28, control 7. |
| risk of viral+ at day 10, 97.2% lower, RR 0.03, p < 0.001, treatment 0 of 28 (0.0%), control 7 of 7 (100.0%), NNT 1.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), primary outcome. | |
| Faisal, 5/10/2021, Randomized Controlled Trial, Pakistan, peer-reviewed, 3 authors, study period 5 April, 2020 - 30 May, 2020, dosage 12mg days 1-5. | risk of no recovery, 68.4% lower, RR 0.32, p = 0.005, treatment 6 of 50 (12.0%), control 19 of 50 (38.0%), NNT 3.8, 6-8 days, mid-recovery, primary outcome. |
| risk of no recovery, 27.3% lower, RR 0.73, p = 0.11, treatment 24 of 50 (48.0%), control 33 of 50 (66.0%), NNT 5.6, 3-5 days. | |
| risk of no recovery, 75.0% lower, RR 0.25, p = 0.09, treatment 2 of 50 (4.0%), control 8 of 50 (16.0%), NNT 8.3, 9-10 days. | |
| Ghauri, 12/15/2020, retrospective, Pakistan, peer-reviewed, 6 authors, dosage 12mg days 1-6. | risk of fever, 92.2% lower, RR 0.08, p = 0.04, treatment 0 of 37 (0.0%), control 7 of 53 (13.2%), NNT 7.6, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 14. |
| risk of fever, 86.4% lower, RR 0.14, p < 0.001, treatment 2 of 37 (5.4%), control 21 of 53 (39.6%), NNT 2.9, day 10. | |
| risk of fever, 55.7% lower, RR 0.44, p < 0.001, treatment 13 of 37 (35.1%), control 42 of 53 (79.2%), NNT 2.3, day 7. | |
| risk of fever, 42.2% lower, RR 0.58, p < 0.001, treatment 21 of 37 (56.8%), control 52 of 53 (98.1%), NNT 2.4, day 5. | Kamal, 9/1/2020, Randomized Controlled Trial, trial NCT04425707 (history). | Estimated 100 patient RCT with results unknown and over 4 years late. |
| Krolewiecki, 6/18/2021, Randomized Controlled Trial, Argentina, peer-reviewed, 23 authors, study period 18 May, 2020 - 9 September, 2020, average treatment delay 3.5 days, dosage 600μg/kg days 1-5, trial NCT004381884 (history). | risk of mechanical ventilation, 151.9% higher, RR 2.52, p = 1.00, treatment 1 of 27 (3.7%), control 0 of 14 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm). |
| risk of progression, 3.7% higher, RR 1.04, p = 1.00, treatment 2 of 27 (7.4%), control 1 of 14 (7.1%). | |
| viral decay rate, RR 0.34, p = 0.09, treatment 20, control 14, relative mean viral decay rate (corrigendum table 2, all treatment patients vs. all control patients), primary outcome. | |
| Loue, 4/17/2021, retrospective quasi-randomized (patient choice), France, peer-reviewed, 2 authors, dosage 200μg/kg single dose. | risk of death, 70.0% lower, RR 0.30, p = 0.34, treatment 1 of 10 (10.0%), control 5 of 15 (33.3%), NNT 4.3. |
| risk of severe case, 55.0% lower, RR 0.45, p = 0.11, treatment 3 of 10 (30.0%), control 10 of 15 (66.7%), NNT 2.7. | |
| López-Medina, 3/4/2021, Double Blind Randomized Controlled Trial, Colombia, peer-reviewed, median age 37.0, 19 authors, study period 15 July, 2020 - 30 November, 2020, average treatment delay 5.0 days, dosage 300μg/kg days 1-5, excluded in exclusion analyses: strong evidence of patients in the control group self-medicating, ivermectin widely used in the population at that time, and the study drug identity was concealed by using the name D11AX22. | risk of death, 66.8% lower, RR 0.33, p = 0.50, treatment 0 of 200 (0.0%), control 1 of 198 (0.5%), NNT 198, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of escalation of care, 60.8% lower, RR 0.39, p = 0.11, treatment 4 of 200 (2.0%), control 10 of 198 (5.1%), NNT 33, odds ratio converted to relative risk. | |
| risk of escalation of care with post-hoc <12h exclusion, 34.3% lower, RR 0.66, p = 0.52, treatment 4 of 200 (2.0%), control 6 of 198 (3.0%), NNT 97, odds ratio converted to relative risk. | |
| risk of deterioration by >= 2 points on an 8-point scale, 43.1% lower, RR 0.57, p = 0.37, treatment 4 of 200 (2.0%), control 7 of 198 (3.5%), NNT 65, odds ratio converted to relative risk, primary outcome. | |
| risk of fever post randomization, 24.8% lower, RR 0.75, p = 0.38, treatment 16 of 200 (8.0%), control 21 of 198 (10.6%), NNT 38, odds ratio converted to relative risk. | |
| risk of unresolved symptoms at day 21, 15.3% lower, RR 0.85, p = 0.53, treatment 36 of 200 (18.0%), control 42 of 198 (21.2%), NNT 31, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, Cox proportional-hazard model. | |
| lack of resolution of symptoms, 6.5% lower, HR 0.93, p = 0.53, treatment 200, control 198, inverted to make HR<1 favor treatment, post-hoc primary outcome. | |
| Mahmud, 10/9/2020, Double Blind Randomized Controlled Trial, Bangladesh, peer-reviewed, 15 authors, study period 1 June, 2020 - 30 August, 2020, average treatment delay 4.0 days, dosage 12mg single dose, this trial uses multiple treatments in the treatment arm (combined with doxycycline) - results of individual treatments may vary, trial NCT04523831 (history). | risk of death, 85.7% lower, HR 0.14, p = 0.25, treatment 0 of 183 (0.0%), control 3 of 183 (1.6%), NNT 61, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of progression, 57.0% lower, HR 0.43, p < 0.001, treatment 16 of 183 (8.7%), control 32 of 180 (17.8%), NNT 11, adjusted per study, Cox regression. | |
| risk of no recovery, 94.0% lower, HR 0.06, p < 0.001, treatment 72 of 183 (39.3%), control 100 of 180 (55.6%), NNT 6.2, adjusted per study, day 7, Cox regression. | |
| risk of no recovery, 38.5% lower, RR 0.61, p = 0.005, treatment 40 of 183 (21.9%), control 64 of 180 (35.6%), NNT 7.3, day 11. | |
| risk of no recovery, 96.0% lower, HR 0.04, p < 0.001, treatment 42 of 183 (23.0%), control 67 of 180 (37.2%), NNT 7.0, adjusted per study, day 12, Cox regression. | |
| time to recovery, 27.0% lower, HR 0.73, p = 0.003, treatment 183, control 180, Cox regression, primary outcome. | |
| risk of no viral clearance, 39.0% lower, HR 0.61, p = 0.002, treatment 14 of 183 (7.7%), control 36 of 180 (20.0%), NNT 8.1, adjusted per study, Cox regression. | |
| Manomaipiboon, 2/2/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Thailand, peer-reviewed, mean age 48.6, 8 authors, study period 10 October, 2021 - 15 December, 2021, dosage 12mg days 1-5, trial NCT05076253 (history). | risk of no recovery, 43.5% lower, RR 0.57, p = 0.26, treatment 3 of 36 (8.3%), control 6 of 36 (16.7%), NNT 12, adjusted per study, odds ratio converted to relative risk, resolution of symptoms, Table S2, day 28. |
| recovery time, 15.3% lower, RR 0.85, p = 0.56, treatment 36, control 36, inverted to make RR<1 favor treatment, time to resolution of symptoms. | |
| risk of no viral clearance, 5.0% lower, RR 0.95, p = 1.00, treatment 19 of 36 (52.8%), control 20 of 36 (55.6%), NNT 36, day 14, primary outcome. | |
| risk of no viral clearance, 3.3% lower, RR 0.97, p = 1.00, treatment 29 of 36 (80.6%), control 30 of 36 (83.3%), NNT 36, day 7. | |
| Mayer, 9/23/2021, retrospective, Argentina, peer-reviewed, 14 authors, dosage 540μg/kg days 1-5, mean prescribed dose. | risk of death, 55.1% lower, RR 0.45, p < 0.001, treatment 3,266, control 17,966, adjusted per study, odds ratio converted to relative risk, Figure 3, multivariable. |
| risk of ICU admission, 65.9% lower, RR 0.34, p < 0.001, treatment 3,266, control 17,966, adjusted per study, odds ratio converted to relative risk, Figure 3, multivariable. | |
| risk of death, 27.6% lower, RR 0.72, p = 0.03, treatment 3,266, control 17,966, odds ratio converted to relative risk, unadjusted. | |
| risk of ICU admission, 26.0% lower, RR 0.74, p = 0.13, treatment 3,266, control 17,966, odds ratio converted to relative risk, unadjusted. | |
| Merino, 5/3/2021, retrospective quasi-randomized (patients receiving kit), population-based cohort, Mexico, preprint, 7 authors, dosage 6mg bid days 1-2. | risk of hospitalization, 74.4% lower, RR 0.26, p < 0.001, model 7, same time period, patients receiving kit. |
| risk of hospitalization, 68.4% lower, RR 0.32, p < 0.001, model 1, different time periods, administrative rule. | |
| Mikamo, 9/26/2022, Double Blind Randomized Controlled Trial, placebo-controlled, multiple countries, peer-reviewed, 19 authors, study period 12 November, 2021 - 7 August, 2022, dosage 300μg/kg days 1-3, trial NCT05056883 (history), excluded in exclusion analyses: very low risk group with almost no progression leaves little room for improvement, unbalanced baseline dyspnea and high symptom scores, design and post-hoc changes favor null result. | COVID-19 pneumonia, 205.0% higher, RR 3.05, p = 0.49, treatment 1 of 502 (0.2%), control 0 of 527 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), Table S8. |
| use of therapeutic agents, oxygen, transfer, hospitalization, death, 214.9% higher, RR 3.15, p = 0.36, treatment 3 of 502 (0.6%), control 1 of 527 (0.2%). | |
| risk of no improvement, 4.0% higher, HR 1.04, p = 0.62, treatment 502, control 527, 168hr, improving trend, primary outcome. | |
| risk of no recovery, 4.0% lower, HR 0.96, p = 0.72, treatment 502, control 527, 168hr, clinical resolution, Figure S3. | |
| risk of no recovery, 4.0% lower, HR 0.96, p = 0.64, treatment 502, control 527, 240hr, clinical resolution, Figure S3. | |
| Mirahmadizadeh, 6/23/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Iran, peer-reviewed, 12 authors, study period 9 April, 2021 - 20 May, 2021, dosage 24mg single dose, 12mg and 24mg arms. | risk of mechanical ventilation, 66.9% lower, RR 0.33, p = 0.37, treatment 1 of 131 (0.8%), control 3 of 130 (2.3%), NNT 65, 24mg. |
| risk of mechanical ventilation, 33.3% lower, RR 0.67, p = 1.00, treatment 2 of 130 (1.5%), control 3 of 130 (2.3%), NNT 130, 12mg. | |
| risk of hospitalization, 45.9% lower, RR 0.54, p = 0.22, treatment 6 of 131 (4.6%), control 11 of 130 (8.5%), NNT 26, 24mg, primary outcome. | |
| risk of hospitalization, 27.3% lower, RR 0.73, p = 0.63, treatment 8 of 130 (6.2%), control 11 of 130 (8.5%), NNT 43, 12mg, primary outcome. | |
| risk of no recovery, 38.9% lower, RR 0.61, p = 0.27, treatment 8 of 131 (6.1%), control 13 of 130 (10.0%), NNT 26, day 28, 24mg. | |
| risk of no recovery, 30.8% lower, RR 0.69, p = 0.50, treatment 9 of 130 (6.9%), control 13 of 130 (10.0%), NNT 32, day 28, 12mg. | |
| Mohan, 2/2/2021, Double Blind Randomized Controlled Trial, India, peer-reviewed, 27 authors, study period 28 July, 2020 - 29 September, 2020, average treatment delay 5.0 days, dosage 400μg/kg single dose, 200μg/kg also tested, trial CTRI/2020/06/026001 (RIVET-COV). | risk of no discharge at day 14, 62.5% lower, RR 0.38, p = 0.27, treatment 2 of 40 (5.0%), control 6 of 45 (13.3%), NNT 12, 24mg. |
| risk of clinical worsening, 32.5% lower, RR 0.68, p = 0.72, treatment 3 of 40 (7.5%), control 5 of 45 (11.1%), NNT 28, 24mg. | |
| risk of no viral clearance, 23.8% lower, RR 0.76, p = 0.18, treatment 21 of 40 (52.5%), control 31 of 45 (68.9%), NNT 6.1, day 5, 24mg, primary outcome. | |
| risk of no viral clearance, 10.3% lower, RR 0.90, p = 0.65, treatment 20 of 36 (55.6%), control 26 of 42 (61.9%), NNT 16, day 7, 24mg. | |
| Mourya, 4/1/2021, retrospective, India, peer-reviewed, 5 authors, dosage 12mg days 1-7. | risk of no viral clearance, 89.4% lower, RR 0.11, p < 0.001, treatment 5 of 50 (10.0%), control 47 of 50 (94.0%), NNT 1.2, primary outcome. |
| Ravikirti (B), 1/9/2021, Double Blind Randomized Controlled Trial, India, peer-reviewed, 11 authors, study period 1 August, 2020 - 31 October, 2020, average treatment delay 6.1 days, dosage 12mg days 1, 2. | risk of death, 88.7% lower, RR 0.11, p = 0.12, treatment 0 of 55 (0.0%), control 4 of 57 (7.0%), NNT 14, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of mechanical ventilation, 79.3% lower, RR 0.21, p = 0.10, treatment 1 of 55 (1.8%), control 5 of 57 (8.8%), NNT 14. | |
| risk of ICU admission, 13.6% lower, RR 0.86, p = 0.80, treatment 5 of 55 (9.1%), control 6 of 57 (10.5%), NNT 70. | |
| risk of no hospital discharge, 88.7% lower, RR 0.11, p = 0.12, treatment 0 of 55 (0.0%), control 4 of 57 (7.0%), NNT 14, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). | |
| risk of no viral clearance, 11.6% higher, RR 1.12, p = 0.35, treatment 42 of 55 (76.4%), control 39 of 57 (68.4%). | |
| Reis, 8/6/2021, Double Blind Randomized Controlled Trial, Brazil, peer-reviewed, 27 authors, study period 23 March, 2021 - 6 August, 2021, dosage 400μg/kg days 1-3, impossible data, see notes, trial NCT04727424 (history) (TOGETHER), excluded in exclusion analyses: multiple anomalies as per detailed analysis. | risk of death, 12.0% lower, RR 0.88, p = 0.68, treatment 21 of 679 (3.1%), control 24 of 679 (3.5%), NNT 226. |
| risk of mechanical ventilation, 23.0% lower, RR 0.77, p = 0.38, treatment 19 of 679 (2.8%), control 25 of 679 (3.7%), NNT 113. | |
| risk of hospitalization, 17.0% lower, RR 0.83, p = 0.19, treatment 79 of 679 (11.6%), control 95 of 679 (14.0%), NNT 42. | |
| extended ER observation or hospitalization, 10.0% lower, RR 0.90, p = 0.42, treatment 100 of 679 (14.7%), control 111 of 679 (16.3%), NNT 62, primary outcome. | |
| viral clearance, no change, RR 1.00, p = 1.00, treatment 106 of 142 (74.6%), control 123 of 165 (74.5%), day 7. | |
| viral clearance, 31.6% higher, RR 1.32, p = 0.46, treatment 148, control 170, inverted to make RR<1 favor treatment, day 3. | |
| Rezai, 6/16/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Iran, peer-reviewed, mean age 35.5, 29 authors, study period 19 February, 2021 - 30 August, 2021, dosage 400μg/kg days 1-3, trial IRCT20111224008507N4, excluded in exclusion analyses: multiple critical issues, see study page. | risk of death, 4.9% higher, RR 1.05, p = 1.00, treatment 1 of 268 (0.4%), control 1 of 281 (0.4%). |
| risk of ICU admission, 9.0% higher, RR 1.09, p = 0.95, treatment 268, control 281. | |
| risk of hospitalization, 36.0% higher, RR 1.36, p = 0.41, treatment 268, control 281. | |
| risk of no recovery, 2.0% higher, RR 1.02, p = 0.49, treatment 268, control 281, inverted to make RR<1 favor treatment, post-hoc primary outcome. | |
| risk of no recovery, 13.2% lower, RR 0.87, p = 0.09, treatment mean 3.87 (±0.18) n=268, control mean 4.46 (±0.18) n=281, cough. | |
| risk of no recovery, 16.7% lower, RR 0.83, p = 0.81, treatment mean 2.5 (±0.51) n=268, control mean 3.0 (±0.92) n=281, tachypnea. | |
| risk of no viral clearance, 23.5% higher, RR 1.23, p = 0.16, treatment 268, control 281, inverted to make RR<1 favor treatment. | |
| Roy, 3/12/2021, retrospective, database analysis, India, preprint, 5 authors, dosage not specified, this trial uses multiple treatments in the treatment arm (combined with doxycycline) - results of individual treatments may vary, excluded in exclusion analyses: no serious outcomes reported and fast recovery in treatment and control groups, there is little room for a treatment to improve results. | relative time to clinical response of wellbeing, 5.6% lower, relative time 0.94, p = 0.87, treatment 14, control 15, primary outcome. |
| Schilling, 7/19/2022, Randomized Controlled Trial, Thailand, peer-reviewed, median age 27.0, 38 authors, study period 30 September, 2021 - 18 April, 2022, average treatment delay 2.0 days, dosage 600μg/kg days 1-7, trial NCT05041907 (history) (PLATCOV), excluded in exclusion analyses: post-hoc change to exclude patients treated before high viral load, population very low risk, recovering quickly without treatment, high baseline immunity, 2.2x greater baseline antibody negative for the treatment arm. | risk of hospitalization, 66.7% lower, RR 0.33, p = 1.00, treatment 0 of 45 (0.0%), control 1 of 45 (2.2%), NNT 45, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of progression, 85.7% lower, RR 0.14, p = 0.24, treatment 0 of 45 (0.0%), control 3 of 45 (6.7%), NNT 15, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), hospitalization or progression to COVID-19 rhabdomyolysis. | |
| relative clearance rate, 9.1% worse, RR 1.09, p = 0.36, treatment 45, control 45, primary outcome. | |
| Siripongboonsitti, 3/29/2024, Randomized Controlled Trial, Thailand, peer-reviewed, 5 authors, study period 7 December, 2022 - 3 February, 2023, dosage 600μg/kg days 1-5, this trial uses multiple treatments in the treatment arm (combined with niclosamide) - results of individual treatments may vary, trial TCTR20230403007 (FINCOV), excluded in exclusion analyses: data consistency issues, very low risk patients/variants with almost no progression, all patients received known effective antiviral, baseline differences. | risk of progression, no change, RR 1.00, p = 1.00, treatment 1 of 30 (3.3%), control 1 of 30 (3.3%), chest xray progression, day 6. |
| risk of progression, 66.7% lower, RR 0.33, p = 1.00, treatment 0 of 30 (0.0%), control 1 of 30 (3.3%), NNT 30, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), chest xray progression, day 3. | |
| risk of no recovery, 39.4% lower, RR 0.61, p = 0.19, treatment 30, control 30, combined symptoms. | |
| risk of no recovery, 70.0% lower, RR 0.30, p = 0.048, treatment 30, control 30, mid-recovery, day 3, cough. | |
| risk of no recovery, 14.3% lower, RR 0.86, p = 0.38, treatment 30, control 30, mid-recovery, day 3, sore throat. | |
| risk of no recovery, 66.7% lower, RR 0.33, p = 0.41, treatment 30, control 30, inverted to make RR<1 favor treatment, mid-recovery, day 3, runny nose. | |
| risk of no recovery, 50.0% lower, RR 0.50, p = 0.32, treatment 30, control 30, inverted to make RR<1 favor treatment, day 6, cough. | |
| relative Ct improvement, 6.1% better, RR 0.94, p = 0.75, treatment median 9.15 IQR 9.7 n=30, control median 8.59 IQR 8.24 n=30, E gene, mid-recovery, day 5, primary outcome. | |
| Szente Fonseca, 10/31/2020, retrospective, Brazil, peer-reviewed, mean age 50.6, 10 authors, average treatment delay 4.6 days, dosage 12mg days 1-2, excluded in exclusion analyses: result is likely affected by collinearity across treatments in the model. | risk of hospitalization, 13.9% higher, RR 1.14, p = 0.53, treatment 340, control 377, adjusted per study, odds ratio converted to relative risk, control prevalence approximated with overall prevalence, primary outcome. |
| Vallejos, 7/2/2021, Double Blind Randomized Controlled Trial, Argentina, peer-reviewed, 29 authors, study period 19 August, 2020 - 22 February, 2021, average treatment delay 4.0 days, dosage 12mg days 1-2, <80kg 12mg, 80-110kg 18mg, >110kg 24mg. | risk of death, 33.5% higher, RR 1.33, p = 0.70, treatment 4 of 250 (1.6%), control 3 of 251 (1.2%), odds ratio converted to relative risk. |
| risk of mechanical ventilation, 33.5% higher, RR 1.33, p = 0.70, treatment 4 of 250 (1.6%), control 3 of 251 (1.2%), odds ratio converted to relative risk. | |
| risk of hospitalization, 33.0% lower, RR 0.67, p = 0.23, treatment 14 of 250 (5.6%), control 21 of 251 (8.4%), NNT 36, odds ratio converted to relative risk, primary outcome. | |
| risk of no viral clearance, 5.0% higher, RR 1.05, p = 0.55, treatment 137 of 250 (54.8%), control 131 of 251 (52.2%), inverted to make RR<1 favor treatment, odds ratio converted to relative risk, day 3. | |
| risk of no viral clearance, 26.8% higher, RR 1.27, p = 0.29, treatment 38 of 250 (15.2%), control 30 of 251 (12.0%), inverted to make RR<1 favor treatment, odds ratio converted to relative risk, day 12. | |
| Wijewickrema, 7/22/2024, Double Blind Randomized Controlled Trial, Sri Lanka, peer-reviewed, 11 authors, study period 29 July, 2021 - 17 March, 2022, dosage 24mg days 1-5, trial SLCTR/2021/020. | risk of death, 196.1% higher, RR 2.96, p = 1.00, treatment 1 of 127 (0.8%), control 0 of 122 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm). |
| progression to moderate disease, 52.0% lower, RR 0.48, p = 0.62, treatment 1 of 127 (0.8%), control 2 of 122 (1.6%), NNT 117, progression to moderate disease. | |
| viral load, 51.2% lower, relative load 0.49, p = 0.03, treatment 80, control 81, relative viral load (copies/mL), day 10, primary outcome. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| Abd-Elsalam, 6/2/2021, Randomized Controlled Trial, Egypt, peer-reviewed, 16 authors, study period March 2020 - October 2020, dosage 12mg days 1-3. | risk of death, 25.0% lower, RR 0.75, p = 0.70, treatment 3 of 82 (3.7%), control 4 of 82 (4.9%), NNT 82, odds ratio converted to relative risk, logistic regression, primary outcome. |
| risk of mechanical ventilation, no change, RR 1.00, p = 1.00, treatment 3 of 82 (3.7%), control 3 of 82 (3.7%). | |
| hospitalization time, 19.6% lower, relative time 0.80, p = 0.09, treatment 82, control 82. | |
| Ahsan, 4/29/2021, retrospective, Pakistan, peer-reviewed, 10 authors, dosage 150μg/kg days 1-2, 150-200µg/kg, this trial uses multiple treatments in the treatment arm (combined with doxycycline) - results of individual treatments may vary, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 50.0% lower, RR 0.50, p = 0.03, treatment 17 of 110 (15.5%), control 17 of 55 (30.9%), NNT 6.5. |
| Aref (B), 9/19/2022, Randomized Controlled Trial, placebo-controlled, Egypt, peer-reviewed, 9 authors, study period 1 March, 2021 - 30 April, 2021, dosage 2 puffs of 70 μg/mL nasal ivermectin, trial NCT04951362 (history). | recovery time, 74.0% lower, relative time 0.26, p < 0.001, treatment 49, control 47, anosmia. |
| Baguma, 12/28/2021, retrospective, Uganda, preprint, 16 authors, study period March 2020 - October 2021, dosage not specified. | risk of death, 96.8% lower, RR 0.03, p = 0.31, treatment 7, control 474, adjusted per study, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, multivariable, control prevalance approximated with overall prevalence. |
| Beltran Gonzalez, 2/23/2021, Double Blind Randomized Controlled Trial, Mexico, peer-reviewed, mean age 53.8, 13 authors, average treatment delay 7.0 days, dosage 12mg single dose, 18mg for patients >80kg, excluded in exclusion analyses: major inconsistencies reported and the data is no longer available, although the authors state that it is available, and have shared it with an anti-treatment group. | risk of death, 14.4% lower, RR 0.86, p = 1.00, treatment 5 of 36 (13.9%), control 6 of 37 (16.2%), NNT 43. |
| risk of respiratory deterioration or death, 8.6% lower, RR 0.91, p = 1.00, treatment 8 of 36 (22.2%), control 9 of 37 (24.3%), NNT 48. | |
| risk of no hospital discharge, 37.0% higher, RR 1.37, p = 0.71, treatment 4 of 36 (11.1%), control 3 of 37 (8.1%). | |
| hospitalization time, 20.0% higher, relative time 1.20, p = 0.43, treatment 36, control 37, primary outcome. | |
| Budhiraja, 11/18/2020, retrospective, India, preprint, 12 authors, dosage not specified. | risk of death, 99.1% lower, RR 0.009, p = 0.04, treatment 0 of 34 (0.0%), control 103 of 942 (10.9%), NNT 9.1, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), unadjusted, primary outcome. |
| Camprubí, 11/11/2020, retrospective, Spain, peer-reviewed, 9 authors, average treatment delay 12.0 days, dosage 200μg/kg single dose. | risk of mechanical ventilation, 40.0% lower, RR 0.60, p = 0.67, treatment 3 of 13 (23.1%), control 5 of 13 (38.5%), NNT 6.5. |
| risk of ICU admission, 33.3% lower, RR 0.67, p = 1.00, treatment 2 of 13 (15.4%), control 3 of 13 (23.1%), NNT 13, ICU at day 8. | |
| risk of no improvement at day 8, 33.3% higher, RR 1.33, p = 1.00, treatment 4 of 13 (30.8%), control 3 of 13 (23.1%). | |
| risk of no viral clearance, 25.0% higher, RR 1.25, p = 1.00, treatment 5 of 13 (38.5%), control 4 of 13 (30.8%), tests done between days 3-5, primary outcome. | |
| Chachar, 9/30/2020, Randomized Controlled Trial, India, peer-reviewed, 6 authors, dosage 36mg, 12mg stat, 12mg after 12 hours, 12mg after 24 hours. | risk of no recovery at day 7, 10.0% lower, RR 0.90, p = 0.50, treatment 9 of 25 (36.0%), control 10 of 25 (40.0%), NNT 25, primary outcome. |
| Efimenko, 2/28/2022, retrospective, propensity score matching, USA, peer-reviewed, 6 authors, study period 1 January, 2020 - 11 July, 2021, dosage not specified, this trial compares with another treatment - results may be better when compared to placebo. | risk of death, 69.2% lower, OR 0.31, p < 0.001, treatment 1,072, control 40,536, propensity score matching, RR approximated with OR. |
| Elavarasi, 8/12/2021, retrospective, India, peer-reviewed, 31 authors, study period April 2021 - June 2021, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 19.6% lower, RR 0.80, p = 0.12, treatment 48 of 283 (17.0%), control 311 of 1,475 (21.1%), NNT 24, unadjusted. |
| Ferreira, 11/26/2021, retrospective, Brazil, peer-reviewed, 5 authors, study period 12 March, 2020 - 8 July, 2020, average treatment delay 7.0 days, dosage not specified, excluded in exclusion analyses: unadjusted results with no group details; substantial unadjusted confounding by indication likely. | risk of death, 5.0% higher, RR 1.05, p = 1.00, treatment 3 of 21 (14.3%), control 11 of 81 (13.6%). |
| risk of death/intubation, 54.3% higher, RR 1.54, p = 0.37, treatment 6 of 21 (28.6%), control 15 of 81 (18.5%). | |
| risk of death/intubation/ICU, 62.4% higher, RR 1.62, p = 0.27, treatment 8 of 21 (38.1%), control 19 of 81 (23.5%). | |
| George, 5/27/2022, Randomized Controlled Trial, India, peer-reviewed, 15 authors, study period June 2020 - February 2021, dosage 24mg single dose, trial CTRI/2020/05/025068. | risk of death, 30.4% lower, RR 0.70, p = 0.55, treatment 5 of 35 (14.3%), control 8 of 39 (20.5%), NNT 16, 24mg. |
| risk of death, 2.6% higher, RR 1.03, p = 1.00, treatment 8 of 38 (21.1%), control 8 of 39 (20.5%), 12mg. | |
| recovery time, 18.7% lower, relative time 0.81, p = 0.37, treatment mean 4.82 (±4.35) n=35, control mean 5.93 (±5.93) n=39, 24mg. | |
| recovery time, 6.2% lower, relative time 0.94, p = 0.78, treatment mean 5.56 (±5.42) n=38, control mean 5.93 (±5.93) n=39, 12mg. | |
| risk of progression, 33.1% lower, RR 0.67, p = 0.41, treatment 6 of 35 (17.1%), control 10 of 39 (25.6%), NNT 12, 24mg. | |
| risk of progression, 17.9% lower, RR 0.82, p = 0.79, treatment 8 of 38 (21.1%), control 10 of 39 (25.6%), NNT 22, 12mg. | |
| Gorial, 7/8/2020, retrospective, Iraq, preprint, 9 authors, dosage 200μg/kg single dose, trial NCT04343092 (history). | risk of death, 71.0% lower, RR 0.29, p = 1.00, treatment 0 of 16 (0.0%), control 2 of 71 (2.8%), NNT 36, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| hospitalization time, 42.0% lower, relative time 0.58, p < 0.001, treatment 16, control 71. | |
| risk of no recovery, 71.0% lower, RR 0.29, p = 1.00, treatment 0 of 16 (0.0%), control 2 of 71 (2.8%), NNT 36, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), primary outcome. | |
| Hashim, 10/26/2020, Single Blind Randomized Controlled Trial, Iraq, peer-reviewed, 7 authors, study period 1 July, 2020 - 14 October, 2020, dosage 200μg/kg days 1-2, some patients received a third dose on day 8, this trial uses multiple treatments in the treatment arm (combined with doxycycline) - results of individual treatments may vary, trial NCT04591600 (history). | risk of death, 91.7% lower, RR 0.08, p = 0.03, treatment 0 of 59 (0.0%), control 6 of 70 (8.6%), NNT 12, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), excluding non-randomized critical patients, primary outcome. |
| risk of death, 67.1% lower, RR 0.33, p = 0.16, treatment 2 of 70 (2.9%), control 6 of 70 (8.6%), NNT 18, odds ratio converted to relative risk, including critical patients that were always allocated to treatment. | |
| risk of progression, 83.1% lower, RR 0.17, p = 0.07, treatment 1 of 59 (1.7%), control 7 of 70 (10.0%), NNT 12, excluding non-randomized critical patients. | |
| risk of progression, 57.4% lower, RR 0.43, p = 0.20, treatment 3 of 70 (4.3%), control 7 of 70 (10.0%), NNT 18, odds ratio converted to relative risk, including critical patients that were always allocated to treatment. | |
| recovery time, 40.7% lower, relative time 0.59, p < 0.001, treatment 70, control 70. | |
| Hashmi, 6/13/2024, Randomized Controlled Trial, Pakistan, preprint, 2 authors, study period 11 June, 2021 - 9 September, 2022, dosage 200μg/kg days 1-5, trial NCT02735707 (history) (REMAP-CAP), excluded in exclusion analyses: baseline severity favors control, post-hoc outcome and SAP changes, see discussion. | risk of death, 14.9% lower, RR 0.85, p = 0.64, treatment 81, control 69, adjusted per study, non-critical/critical combined. |
| risk of death, 22.5% lower, OR 0.78, p = 0.59, treatment 44, control 45, adjusted per study, inverted to make OR<1 favor treatment, non-critical, day 90, RR approximated with OR. | |
| risk of death, 5.7% lower, OR 0.94, p = 0.91, treatment 37, control 24, adjusted per study, inverted to make OR<1 favor treatment, critical, day 90, RR approximated with OR. | |
| intubation, ECMO, death, 23.7% lower, OR 0.76, p = 0.57, treatment 44, control 45, adjusted per study, inverted to make OR<1 favor treatment, non-critical, RR approximated with OR. | |
| intubation, ECMO, death, 16.0% lower, OR 0.84, p = 0.72, treatment 37, control 24, adjusted per study, inverted to make OR<1 favor treatment, critical, RR approximated with OR. | |
| organ support-free days, 3.8% lower, OR 0.96, p = 0.93, treatment 44, control 45, inverted to make OR<1 favor treatment, non-critical, RR approximated with OR. | |
| organ support-free days, 6.4% higher, OR 1.06, p = 0.89, treatment 37, control 24, inverted to make OR<1 favor treatment, critical, RR approximated with OR. | |
| Hayward, 2/29/2024, Randomized Controlled Trial, placebo-controlled, United Kingdom, peer-reviewed, 25 authors, study period 23 June, 2021 - 1 July, 2022, dosage 350μg/kg days 1-3, trial ISRCTN86534580 (PRINCIPLE). | risk of death/hospitalization, 1.0% higher, HR 1.01, p = 0.97, treatment 34 of 2,157 (1.6%), control 27 of 1,806 (1.5%), concurrent and eligible, primary outcome. |
| risk of mechanical ventilation, 151.4% higher, RR 2.51, p = 0.63, treatment 3 of 2,149 (0.1%), control 1 of 1,801 (0.1%). | |
| risk of ICU admission, 319.0% higher, RR 4.19, p = 0.23, treatment 5 of 2,149 (0.2%), control 1 of 1,801 (0.1%). | |
| time to sustained recovery, 16.0% lower, HR 0.84, p < 0.001, treatment 2,157, control 1,806, inverted to make HR<1 favor treatment, concurrent and eligible. | |
| early sustained recovery, 23.1% lower, HR 0.77, p < 0.001, treatment 2,154, control 1,805, inverted to make HR<1 favor treatment, concurrent and eligible. | |
| sustained alleviation, 17.4% lower, HR 0.83, p < 0.001, treatment 1,826, control 1,535, inverted to make HR<1 favor treatment, concurrent and eligible. | |
| alleviation of all symptoms, 16.0% lower, HR 0.84, p < 0.001, treatment 2,154, control 1,805, inverted to make HR<1 favor treatment, concurrent and eligible. | |
| first reported recovery, 13.0% lower, HR 0.87, p < 0.001, treatment 2,157, control 1,806, inverted to make HR<1 favor treatment, concurrent and eligible, primary outcome. | |
| no recovery at 3/6/12 months, 28.0% lower, HR 0.72, p = 0.02, treatment 94 of 1,941 (4.8%), control 109 of 1,624 (6.7%), NNT 54. | |
| risk of no recovery, 17.6% lower, RR 0.82, p = 0.001, treatment 417 of 1,848 (22.6%), control 420 of 1,533 (27.4%), NNT 21, day 365. | |
| risk of PASC, 36.3% lower, RR 0.64, p < 0.001, treatment 1,886, control 1,567, all symptoms combined. | |
| risk of PASC, 63.2% higher, RR 1.63, p = 1.00, treatment 2 of 1,507 (0.1%), control 1 of 1,230 (0.1%), ongoing/persistent, fever. | |
| risk of PASC, 72.7% lower, RR 0.27, p = 0.33, treatment 1 of 1,819 (0.1%), control 3 of 1,489 (0.2%), NNT 683, ongoing/persistent, cough. | |
| risk of PASC, 50.1% lower, RR 0.50, p = 0.04, treatment 15 of 1,886 (0.8%), control 25 of 1,567 (1.6%), NNT 125, ongoing/persistent, dyspnea. | |
| risk of PASC, 35.3% higher, RR 1.35, p = 0.74, treatment 5 of 1,808 (0.3%), control 3 of 1,468 (0.2%), ongoing/persistent, chest pain. | |
| risk of PASC, 25.2% lower, RR 0.75, p = 0.36, treatment 21 of 1,831 (1.1%), control 23 of 1,501 (1.5%), NNT 259, ongoing/persistent, smell. | |
| risk of PASC, 58.7% lower, RR 0.41, p = 0.42, treatment 2 of 1,821 (0.1%), control 4 of 1,503 (0.3%), NNT 640, ongoing/persistent, diarrhoea. | |
| risk of PASC, 70.2% lower, RR 0.30, p < 0.001, treatment 10 of 1,739 (0.6%), control 27 of 1,400 (1.9%), NNT 74, ongoing/persistent, headache. | |
| risk of PASC, 29.8% lower, RR 0.70, p = 0.25, treatment 23 of 1,739 (1.3%), control 27 of 1,433 (1.9%), NNT 178, ongoing/persistent, muscle ache. | |
| risk of PASC, 47.1% lower, RR 0.53, p = 0.03, treatment 19 of 1,724 (1.1%), control 30 of 1,441 (2.1%), NNT 102, ongoing/persistent, generally unwell. | |
| risk of PASC, 20.1% lower, RR 0.80, p = 0.19, treatment 66 of 1,876 (3.5%), control 69 of 1,567 (4.4%), NNT 113, ongoing/persistent, fatigue. | |
| risk of PASC, 28.5% lower, RR 0.72, p < 0.001, treatment 1,513, control 1,238, adjusted per study, all symptoms combined. | |
| risk of PASC, 39.9% lower, RR 0.60, p = 0.01, treatment 46 of 1,435 (3.2%), control 51 of 1,136 (4.5%), relatedness (yes + unsure) 9.1% (treatment) 11.2% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, cough. | |
| risk of PASC, 41.6% lower, RR 0.58, p < 0.001, treatment 96 of 1,513 (6.3%), control 106 of 1,238 (8.6%), relatedness (yes + unsure) 14.4% (treatment) 18.5% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, shortness of breath. | |
| risk of PASC, 22.2% lower, RR 0.78, p = 0.27, treatment 39 of 1,426 (2.7%), control 36 of 1,117 (3.2%), relatedness (yes + unsure) 7.6% (treatment) 8.4% (control) , NNT 205, adjusted per study and for relatedness, moderate/major symptoms at 12 months, chest pain. | |
| risk of PASC, 38.0% lower, RR 0.62, p = 0.02, treatment 46 of 1,427 (3.2%), control 44 of 1,140 (3.9%), relatedness (yes + unsure) 7.7% (treatment) 10.3% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, palpitations. | |
| risk of PASC, 11.5% higher, RR 1.12, p = 0.52, treatment 77 of 1,403 (5.5%), control 57 of 1,131 (5.0%), relatedness (yes + unsure) 13.2% (treatment) 12.9% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, smell. | |
| risk of PASC, 36.4% lower, RR 0.64, p = 0.02, treatment 51 of 1,375 (3.7%), control 51 of 1,116 (4.6%), relatedness (yes + unsure) 1.1% (treatment) 1.4% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, taste. | |
| risk of PASC, 22.1% lower, RR 0.78, p = 0.37, treatment 26 of 1,290 (2.0%), control 25 of 1,057 (2.4%), relatedness (yes + unsure) 4.8% (treatment) 5.3% (control) , NNT 286, adjusted per study and for relatedness, moderate/major symptoms at 12 months, ear ache. | |
| risk of PASC, 9.6% higher, RR 1.10, p = 0.73, treatment 37 of 1,325 (2.8%), control 25 of 1,089 (2.3%), relatedness (yes + unsure) 6.7% (treatment) 7.4% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, sore throat. | |
| risk of PASC, 34.8% lower, RR 0.65, p = 0.12, treatment 24 of 1,308 (1.8%), control 27 of 1,077 (2.5%), relatedness (yes + unsure) 6.0% (treatment) 6.9% (control) , NNT 149, adjusted per study and for relatedness, moderate/major symptoms at 12 months, hoarse voice. | |
| risk of PASC, 16.6% higher, RR 1.17, p = 0.42, treatment 60 of 1,341 (4.5%), control 46 of 1,082 (4.3%), relatedness (yes + unsure) 8.3% (treatment) 7.4% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, tinnitus. | |
| risk of PASC, 34.7% lower, RR 0.65, p = 0.29, treatment 13 of 1,382 (0.9%), control 12 of 1,139 (1.1%), relatedness (yes + unsure) 2.2% (treatment) 3.0% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, vomiting. | |
| risk of PASC, 46.5% higher, RR 1.46, p = 0.12, treatment 44 of 1,439 (3.1%), control 25 of 1,175 (2.1%), relatedness (yes + unsure) 5.9% (treatment) 5.8% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, abdominal pain. | |
| risk of PASC, 1.6% lower, RR 0.98, p = 0.95, treatment 33 of 1,416 (2.3%), control 24 of 1,167 (2.1%), relatedness (yes + unsure) 4.4% (treatment) 5.1% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, diarrhoea. | |
| risk of PASC, 43.8% higher, RR 1.44, p = 0.23, treatment 30 of 1,417 (2.1%), control 17 of 1,160 (1.5%), relatedness (yes + unsure) 4.5% (treatment) 4.6% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, reduced appetite. | |
| risk of PASC, 89.8% higher, RR 1.90, p = 0.27, treatment 11 of 1,375 (0.8%), control 4 of 1,129 (0.4%), relatedness (yes + unsure) 1.8% (treatment) 2.2% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, weight loss. | |
| risk of PASC, 41.3% lower, RR 0.59, p < 0.001, treatment 89 of 1,287 (6.9%), control 94 of 973 (9.7%), relatedness (yes + unsure) 13.2% (treatment) 16.2% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, anxiety. | |
| risk of PASC, 38.6% lower, RR 0.61, p < 0.001, treatment 95 of 1,298 (7.3%), control 92 of 992 (9.3%), relatedness (yes + unsure) 13.7% (treatment) 17.4% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, depression. | |
| risk of PASC, 49.0% lower, RR 0.51, p < 0.001, treatment 129 of 1,376 (9.4%), control 143 of 1,105 (12.9%), relatedness (yes + unsure) 19.6% (treatment) 27.3% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, brain fog. | |
| risk of PASC, 32.9% lower, RR 0.67, p = 0.08, treatment 37 of 1,187 (3.1%), control 33 of 874 (3.8%), relatedness (yes + unsure) 7.1% (treatment) 9.2% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, confusion. | |
| risk of PASC, 41.9% lower, RR 0.58, p < 0.001, treatment 78 of 1,278 (6.1%), control 81 of 964 (8.4%), relatedness (yes + unsure) 12.5% (treatment) 15.7% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, headache. | |
| risk of PASC, 45.4% lower, RR 0.55, p = 0.001, treatment 53 of 1,254 (4.2%), control 54 of 955 (5.7%), relatedness (yes + unsure) 11.5% (treatment) 15.8% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, dizziness. | |
| risk of PASC, 73.5% lower, RR 0.27, p = 0.10, treatment 3 of 1,105 (0.3%), control 3 of 802 (0.4%), relatedness (yes + unsure) 0.4% (treatment) 1.1% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, fainting. | |
| risk of PASC, 38.7% lower, RR 0.61, p = 0.02, treatment 42 of 1,200 (3.5%), control 39 of 894 (4.4%), relatedness (yes + unsure) 7.9% (treatment) 10.7% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, numbness. | |
| risk of PASC, 42.1% lower, RR 0.58, p < 0.001, treatment 123 of 1,288 (9.5%), control 121 of 982 (12.3%), relatedness (yes + unsure) 13.9% (treatment) 18.5% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, sleeping problems. | |
| risk of PASC, 11.8% lower, RR 0.88, p = 0.37, treatment 99 of 1,180 (8.4%), control 88 of 967 (9.1%), relatedness (yes + unsure) 15.1% (treatment) 16.1% (control) , NNT 141, adjusted per study and for relatedness, moderate/major symptoms at 12 months, body pains. | |
| risk of PASC, 32.2% lower, RR 0.68, p < 0.001, treatment 136 of 1,220 (11.1%), control 146 of 1,034 (14.1%), relatedness (yes + unsure) 16.1% (treatment) 19.0% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, joint pains. | |
| risk of PASC, 30.2% lower, RR 0.70, p < 0.001, treatment 205 of 1,398 (14.7%), control 209 of 1,181 (17.7%), relatedness (yes + unsure) 24.1% (treatment) 28.3% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, fatigue. | |
| risk of PASC, 31.9% lower, RR 0.68, p = 0.006, treatment 91 of 1,208 (7.5%), control 89 of 997 (8.9%), relatedness (yes + unsure) 14.5% (treatment) 18.1% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, weakness. | |
| risk of PASC, 35.9% lower, RR 0.64, p < 0.001, treatment 99 of 1,211 (8.2%), control 107 of 1,002 (10.7%), relatedness (yes + unsure) 14.3% (treatment) 17.4% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, generally unwell. | |
| risk of PASC, 9.2% lower, RR 0.91, p = 0.81, treatment 16 of 1,066 (1.5%), control 11 of 855 (1.3%), relatedness (yes + unsure) 3.0% (treatment) 3.8% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, fever. | |
| risk of PASC, 42.4% lower, RR 0.58, p = 0.21, treatment 10 of 1,065 (0.9%), control 11 of 853 (1.3%), relatedness (yes + unsure) 3.0% (treatment) 3.7% (control) , adjusted per study and for relatedness, moderate/major symptoms at 12 months, rashes. | |
| risk of PASC, 10.0% lower, RR 0.90, p = 0.62, treatment 47 of 1,090 (4.3%), control 41 of 873 (4.7%), NNT 260, adjusted per study, moderate/major symptoms at 12 months, other. | |
| Hazan (B), 7/7/2021, retrospective, USA, preprint, 7 authors, dosage 12mg days 1, 4, 8, this trial uses multiple treatments in the treatment arm (combined with doxycycline, zinc, vitamin D, vitamin C) - results of individual treatments may vary, trial NCT04949230 (history), excluded in exclusion analyses: study uses a synthetic control arm. | risk of death, 86.2% lower, RR 0.14, p = 0.04, NNT 6.9, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of hospitalization, 93.5% lower, RR 0.07, p = 0.001, NNT 3.3, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), primary outcome. | |
| Huvemek, 3/25/2021, Double Blind Randomized Controlled Trial, Bulgaria, preprint, 1 author, average treatment delay 7.0 days, dosage 400μg/kg days 1-3, trial EudraCT2020-002091-12. | risk of no improvement, 31.6% lower, RR 0.68, p = 0.28, treatment 13 of 50 (26.0%), control 19 of 50 (38.0%), NNT 8.3, patients with improvement on WHO scale, day 7. |
| risk of no improvement, 31.8% lower, RR 0.68, p = 0.21, treatment 15 of 50 (30.0%), control 22 of 50 (44.0%), NNT 7.1, patients with improvement on WHO scale, day 6. | |
| risk of no improvement, 36.0% lower, RR 0.64, p = 0.10, treatment 16 of 50 (32.0%), control 25 of 50 (50.0%), NNT 5.6, patients with improvement on WHO scale, day 5. | |
| risk of no improvement, 34.5% lower, RR 0.66, p = 0.07, treatment 19 of 50 (38.0%), control 29 of 50 (58.0%), NNT 5.0, patients with improvement on WHO scale, day 4. | |
| Jamir, 12/13/2021, retrospective, India, peer-reviewed, 6 authors, study period June 2020 - October 2020, dosage not specified. | risk of death, 53.0% higher, RR 1.53, p = 0.13, treatment 32 of 76 (42.1%), control 69 of 190 (36.3%), adjusted per study, multivariable Cox regression. |
| Khan, 9/24/2020, retrospective, Bangladesh, peer-reviewed, median age 35.0, 8 authors, dosage 12mg single dose. | risk of death, 87.1% lower, RR 0.13, p = 0.02, treatment 1 of 115 (0.9%), control 9 of 133 (6.8%), NNT 17. |
| risk of ICU admission, 89.5% lower, RR 0.11, p = 0.007, treatment 1 of 115 (0.9%), control 11 of 133 (8.3%), NNT 14. | |
| risk of progression, 83.5% lower, RR 0.17, p < 0.001, treatment 3 of 115 (2.6%), control 21 of 133 (15.8%), NNT 7.6. | |
| risk of no recovery, 87.1% lower, RR 0.13, p = 0.02, treatment 1 of 115 (0.9%), control 9 of 133 (6.8%), NNT 17. | |
| hospitalization time, 40.0% lower, relative time 0.60, p < 0.001, treatment 115, control 133. | |
| time to viral-, 73.3% lower, relative time 0.27, p < 0.001, treatment 115, control 133. | |
| Kishoria, 8/31/2020, Randomized Controlled Trial, India, peer-reviewed, 7 authors, dosage 12mg single dose, excluded in exclusion analyses: excessive unadjusted differences between groups. | risk of no hospital discharge, 7.5% higher, RR 1.08, p = 1.00, treatment 11 of 19 (57.9%), control 7 of 13 (53.8%). |
| risk of no viral clearance, 7.5% higher, RR 1.08, p = 1.00, treatment 11 of 19 (57.9%), control 7 of 13 (53.8%), day 3, primary outcome. | |
| risk of no viral clearance, 220.0% higher, RR 3.20, p = 0.45, treatment 1 of 5 (20.0%), control 0 of 6 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), day 5. | |
| Lim, 11/3/2021, Randomized Controlled Trial, Malaysia, peer-reviewed, 26 authors, study period 31 May, 2021 - 9 October, 2021, average treatment delay 5.1 days, dosage 400μg/kg days 1-5, trial NCT04920942 (history) (I-TECH). | risk of death, 69.0% lower, RR 0.31, p = 0.09, treatment 3 of 241 (1.2%), control 10 of 249 (4.0%), NNT 36. |
| risk of death, 75.2% lower, RR 0.25, p = 0.02, treatment 3 of 52 (5.8%), control 10 of 43 (23.3%), NNT 5.7, among patients progressing to severe cases (mostly before treatment ended). | |
| risk of mechanical ventilation, 59.0% lower, RR 0.41, p = 0.17, treatment 4 of 241 (1.7%), control 10 of 249 (4.0%), NNT 42. | |
| risk of ICU admission, 22.0% lower, RR 0.78, p = 0.79, treatment 6 of 241 (2.5%), control 8 of 249 (3.2%), NNT 138. | |
| risk of progression, 31.1% lower, RR 0.69, p = 0.29, treatment 14 of 241 (5.8%), control 21 of 249 (8.4%), NNT 38, death/IMV/NIV/high flow (WHO severe cases). | |
| risk of progression, 25.0% higher, RR 1.25, p = 0.25, treatment 52 of 241 (21.6%), control 43 of 249 (17.3%), primary outcome. | |
| hospitalization time, 5.5% higher, relative time 1.05, p = 0.38, treatment 241, control 249. | |
| risk of no recovery, 2.5% higher, RR 1.02, p = 0.86, treatment 116 of 241 (48.1%), control 116 of 247 (47.0%), day 5. | |
| Lima-Morales, 2/10/2021, prospective, Mexico, peer-reviewed, 10 authors, average treatment delay 7.2 days, dosage 12mg single dose, this trial uses multiple treatments in the treatment arm (combined with azithromycin, montelukast, and aspirin) - results of individual treatments may vary. | risk of death, 77.7% lower, RR 0.22, p < 0.001, treatment 15 of 481 (3.1%), control 52 of 287 (18.1%), NNT 6.7, adjusted per study, odds ratio converted to relative risk, multivariate. |
| risk of mechanical ventilation, 51.9% lower, RR 0.48, p = 0.15, treatment 8 of 434 (1.8%), control 11 of 287 (3.8%), NNT 50. | |
| risk of hospitalization, 67.4% lower, RR 0.33, p < 0.001, treatment 44 of 481 (9.1%), control 89 of 287 (31.0%), NNT 4.6, adjusted per study, odds ratio converted to relative risk, multivariate. | |
| risk of no recovery, 58.6% lower, RR 0.41, p < 0.001, treatment 75 of 481 (15.6%), control 118 of 287 (41.1%), NNT 3.9, adjusted per study, inverted to make RR<1 favor treatment, odds ratio converted to relative risk, recovery at day 14 after symptoms, multivariate. | |
| Llenas-García, 5/10/2023, retrospective, Spain, peer-reviewed, 11 authors, study period 23 February, 2020 - 14 March, 2021, average treatment delay 6.0 days, dosage 200μg/kg single dose. | risk of death, 16.7% lower, RR 0.83, p = 0.82, treatment 10 of 96 (10.4%), control 12 of 96 (12.5%), NNT 48. |
| risk of oxygen therapy, 18.4% lower, RR 0.82, p = 0.37, treatment 31 of 96 (32.3%), control 38 of 96 (39.6%), NNT 14. | |
| risk of progression, 23.0% lower, OR 0.77, p = 0.52, treatment 96, control 96, adjusted per study, in-hospital mortality or respiratory support, multivariable, primary outcome, RR approximated with OR. | |
| risk of ICU admission, 4.0% higher, OR 1.04, p = 0.92, treatment 96, control 96, adjusted per study, multivariable, RR approximated with OR. | |
| Munir, 4/21/2023, retrospective, Pakistan, peer-reviewed, 3 authors, study period March 2021 - March 2022, dosage not specified. | risk of death, 48.2% lower, OR 0.52, p = 0.13, treatment 92, control 908, adjusted per study, multivariable, RR approximated with OR. |
| Mustafa, 12/29/2021, retrospective, Pakistan, peer-reviewed, 7 authors, dosage varies, excluded in exclusion analyses: unadjusted results with no group details. | risk of death, 63.7% lower, RR 0.36, p = 0.09, treatment 3 of 73 (4.1%), control 42 of 371 (11.3%), NNT 14. |
| Naggie, 6/12/2022, Double Blind Randomized Controlled Trial, placebo-controlled, USA, peer-reviewed, 28 authors, study period 23 June, 2021 - 4 February, 2022, average treatment delay 6.0 days, dosage 600μg/kg days 1-6, trial NCT04885530 (history) (ACTIV-6). | risk of death, 202.3% higher, RR 3.02, p = 0.49, treatment 1 of 708 (0.1%), control 0 of 724 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), 600µg/kg, day 28. |
| risk of death, 194.7% higher, RR 2.95, p = 1.00, treatment 1 of 817 (0.1%), control 0 of 774 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), 400µg/kg, day 28. | |
| risk of death/hospitalization, 256.9% higher, RR 3.57, p = 0.11, treatment 7 of 708 (1.0%), control 2 of 722 (0.3%), 600µg/kg, day 28. | |
| risk of hospitalization, 5.3% higher, RR 1.05, p = 1.00, treatment 10 of 817 (1.2%), control 9 of 774 (1.2%), 400µg/kg, day 28. | |
| risk of progression, 68.4% lower, RR 0.32, p = 0.36, treatment 1 of 817 (0.1%), control 3 of 774 (0.4%), NNT 377, 400µg/kg, aggravated C19 pneumonia, eTable 2. | |
| risk of progression, 3.0% lower, RR 0.97, p = 0.53, treatment 39 of 708 (5.5%), control 42 of 722 (5.8%), NNT 324, adjusted per study, urgent or emergency care visits, hospitalizations, or death, 600µg/kg. | |
| risk of progression, 20.0% higher, RR 1.20, p = 0.32, treatment 32 of 817 (3.9%), control 28 of 774 (3.6%), adjusted per study, urgent or emergency care visits, hospitalizations, or death, 400µg/kg. | |
| clinical progression, 29.0% higher, OR 1.29, p = 0.30, treatment 708, control 724, mid-recovery, 600µg/kg, day 7, RR approximated with OR. | |
| clinical progression, 150.0% higher, OR 2.50, p = 0.007, treatment 708, control 724, 600µg/kg, day 14, RR approximated with OR. | |
| clinical progression, 150.0% higher, OR 2.50, p = 0.03, treatment 708, control 724, 600µg/kg, day 28, RR approximated with OR. | |
| clinical progression, 24.0% lower, OR 0.76, p = 0.07, treatment 817, control 774, mid-recovery, 400µg/kg, day 7, RR approximated with OR. | |
| clinical progression, 27.0% lower, OR 0.73, p = 0.05, treatment 817, control 774, 400µg/kg, day 14, RR approximated with OR. | |
| clinical progression, 10.0% lower, OR 0.90, p = 0.57, treatment 817, control 774, 400µg/kg, day 28, RR approximated with OR. | |
| time to recovery, 2.0% lower, HR 0.98, p = 0.71, treatment 708, control 724, inverted to make HR<1 favor treatment, 600µg/kg, post-hoc primary outcome. | |
| risk of limited activity, 30.5% lower, RR 0.70, p = 0.14, treatment 30 of 805 (3.7%), control 41 of 765 (5.4%), NNT 61, eFigure 2, 400µg/kg, day 14. | |
| time to recovery, 6.5% lower, HR 0.93, p = 0.18, treatment 817, control 774, inverted to make HR<1 favor treatment, 400µg/kg, post-hoc primary outcome. | |
| time to recovery, 46.2% lower, HR 0.54, p = 0.02, treatment 39, control 51, inverted to make HR<1 favor treatment, 400µg/kg, severe, recovery. | |
| Ochoa-Jaramillo, 10/21/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Colombia, peer-reviewed, 8 authors, study period 10 December, 2020 - 9 December, 2021, average treatment delay 8.8 days, dosage 400μg/kg single dose, trial NCT04602507 (history). | risk of death, 57.0% lower, HR 0.43, p = 0.35, treatment 2 of 37 (5.4%), control 4 of 38 (10.5%), NNT 20, Cox proportional hazards. |
| risk of mechanical ventilation, 34.0% higher, HR 1.34, p = 0.62, treatment 7 of 37 (18.9%), control 5 of 38 (13.2%), Cox proportional hazards. | |
| risk of ICU admission, 37.0% higher, HR 1.37, p = 0.52, treatment 8 of 37 (21.6%), control 6 of 38 (15.8%), Cox proportional hazards, primary outcome. | |
| Okumuş, 1/12/2021, Double Blind Randomized Controlled Trial, Turkey, peer-reviewed, 15 authors, study period May 2020 - September 2020, dosage 200μg/kg days 1-5, 36-50kg - 9mg, 51-65kg - 12mg, 66-79kg - 15mg, >80kg 200μg/kg, trial NCT04646109 (history). | risk of death, 33.3% lower, RR 0.67, p = 0.55, treatment 6 of 30 (20.0%), control 9 of 30 (30.0%), NNT 10. |
| risk of no improvement at day 10, 42.9% lower, RR 0.57, p = 0.18, treatment 8 of 30 (26.7%), control 14 of 30 (46.7%), NNT 5.0. | |
| risk of no improvement at day 5, 15.8% lower, RR 0.84, p = 0.60, treatment 16 of 30 (53.3%), control 19 of 30 (63.3%), NNT 10, primary outcome. | |
| risk of no viral clearance, 80.0% lower, RR 0.20, p = 0.02, treatment 2 of 16 (12.5%), control 5 of 8 (62.5%), NNT 2.0, day 10. | |
| Osati, 7/16/2023, retrospective, Tanzania, preprint, median age 60.0, 22 authors, study period 26 March, 2021 - 30 July, 2022, dosage not specified. | risk of death, 31.5% lower, OR 0.68, p = 0.02, treatment 448, control 849, adjusted per study, inverted to make OR<1 favor treatment, multivariable, RR approximated with OR. |
| Ozer, 11/23/2021, prospective, USA, peer-reviewed, 12 authors, dosage 200μg/kg days 1, 3. | risk of death, 75.0% lower, RR 0.25, p = 0.09, treatment 2 of 60 (3.3%), control 8 of 60 (13.3%), NNT 10.0, PSM. |
| risk of mechanical ventilation, 12.6% lower, RR 0.87, p = 0.20, treatment 3 of 60 (5.0%), control 2 of 60 (3.3%), adjusted per study, odds ratio converted to relative risk, propensity score matching, multivariable. | |
| ventilation time, 83.3% lower, relative time 0.17, p = 0.002, treatment 60, control 60. | |
| risk of ICU admission, 48.7% lower, RR 0.51, p = 0.42, treatment 6 of 60 (10.0%), control 3 of 60 (5.0%), adjusted per study, odds ratio converted to relative risk, propensity score matching, multivariable. | |
| ICU time, 70.6% lower, relative time 0.29, p < 0.001, treatment 60, control 60. | |
| hospitalization time, 9.0% higher, relative time 1.09, p = 0.09, treatment 60, control 60, adjusted per study, propensity score matching, multivariable. | |
| Podder, 9/3/2020, Randomized Controlled Trial, Bangladesh, peer-reviewed, 4 authors, study period 1 May, 2020 - 31 July, 2020, average treatment delay 7.0 days, dosage 200μg/kg single dose. | recovery time from enrollment, 16.1% lower, relative time 0.84, p = 0.34, treatment 32, control 30. |
| Pott-Junior, 3/9/2021, Randomized Controlled Trial, Brazil, peer-reviewed, 10 authors, study period 1 July, 2020 - 1 December, 2020, average treatment delay 8.0 days, dosage 200μg/kg single dose, dose varies in three arms 100, 200, 400μg/kg, trial NCT04431466 (history). | risk of mechanical ventilation, 85.2% lower, RR 0.15, p = 0.25, treatment 1 of 27 (3.7%), control 1 of 4 (25.0%), NNT 4.7. |
| risk of ICU admission, 85.2% lower, RR 0.15, p = 0.25, treatment 1 of 27 (3.7%), control 1 of 4 (25.0%), NNT 4.7. | |
| relative improvement in Ct value, 0.8% better, RR 0.99, p = 1.00, treatment 27, control 3. | |
| risk of no viral clearance, 11.1% higher, RR 1.11, p = 1.00, treatment 10 of 27 (37.0%), control 1 of 3 (33.3%), primary outcome. | |
| Qadeer, 8/31/2022, prospective, Pakistan, peer-reviewed, median age 55.4, 6 authors, study period 1 November, 2020 - 30 May, 2021, dosage 12mg days 1-5, excluded in exclusion analyses: minimal baseline details provided. | risk of no viral clearance, 58.3% lower, RR 0.42, p < 0.001, treatment 35 of 105 (33.3%), control 84 of 105 (80.0%), NNT 2.1, mid-recovery, day 10. |
| risk of no viral clearance, 20.0% lower, RR 0.80, p < 0.001, treatment 84 of 105 (80.0%), control 105 of 105 (100.0%), NNT 5.0, day 7. | |
| risk of no viral clearance, 98.6% lower, RR 0.01, p < 0.001, treatment 0 of 105 (0.0%), control 35 of 105 (33.3%), NNT 3.0, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), day 14. | |
| Rajter, 10/13/2020, retrospective, propensity score matching, USA, peer-reviewed, 6 authors, dosage 200μg/kg single dose. | risk of death, 46.0% lower, RR 0.54, p = 0.045, treatment 13 of 98 (13.3%), control 24 of 98 (24.5%), NNT 8.9, adjusted per study, odds ratio converted to relative risk, PSM. |
| risk of death, 66.9% lower, RR 0.33, p = 0.03, treatment 26 of 173 (15.0%), control 27 of 107 (25.2%), NNT 9.8, adjusted per study, odds ratio converted to relative risk, multivariate, primary outcome. | |
| risk of mechanical ventilation, 63.6% lower, RR 0.36, p = 0.10, treatment 4 of 98 (4.1%), control 11 of 98 (11.2%), NNT 14, matched cohort excluding intubated at baseline. | |
| Ravikirti, 4/6/2022, retrospective, India, preprint, 7 authors, study period 1 April, 2021 - 15 May, 2021, dosage varies, excluded in exclusion analyses: exclusion of patients in less severe condition, data/analysis concerns. | risk of death, 2.8% lower, RR 0.97, p = 0.82, treatment 53 of 171 (31.0%), control 254 of 794 (32.0%), NNT 100, odds ratio converted to relative risk. |
| Rezai (B), 6/16/2022, Double Blind Randomized Controlled Trial, placebo-controlled, Iran, peer-reviewed, mean age 53.8, 29 authors, study period 19 February, 2021 - 14 August, 2021, average treatment delay 7.18 days, dosage 400μg/kg days 1-3, trial IRCT20111224008507N5, excluded in exclusion analyses: multiple critical issues, see study page. | risk of death, 30.8% lower, RR 0.69, p = 0.36, treatment 13 of 311 (4.2%), control 18 of 298 (6.0%), NNT 54. |
| risk of mechanical ventilation, 50.0% lower, RR 0.50, p = 0.07, treatment 311, control 298. | |
| risk of ICU admission, 16.0% lower, RR 0.84, p = 0.47, treatment 311, control 298. | |
| hospitalization time, 11.5% higher, relative time 1.11, p = 0.009, treatment mean 7.98 (±4.4) n=311, control mean 7.16 (±3.2) n=298. | |
| deterioration, 12.7% higher, RR 1.13, p = 0.74, treatment 20 of 311 (6.4%), control 17 of 298 (5.7%). | |
| risk of no recovery, 24.2% lower, RR 0.76, p = 0.02, treatment 311, control 298, inverted to make RR<1 favor treatment, post-hoc primary outcome. | |
| risk of no recovery, 64.0% lower, RR 0.36, p = 0.06, treatment 5 of 145 (3.4%), control 10 of 105 (9.5%), NNT 16, day 7, cough. | |
| risk of no recovery, 76.0% lower, RR 0.24, p = 0.38, day 7, tachypnea. | |
| Rezk, 10/30/2021, prospective, Egypt, peer-reviewed, 4 authors, dosage 36mg days 1, 3, 6. | risk of death, 80.0% lower, RR 0.20, p = 0.50, treatment 0 of 160 (0.0%), control 2 of 160 (1.2%), NNT 80, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of progression, 55.6% lower, RR 0.44, p = 0.06, treatment 8 of 160 (5.0%), control 18 of 160 (11.2%), NNT 16, 2 weeks, including deaths. | |
| risk of no recovery, 33.4% lower, RR 0.67, p = 0.27, treatment 14 of 145 (9.7%), control 20 of 138 (14.5%), NNT 21, 4 weeks, more patients were lost to followup in the control group. | |
| time to viral-, 27.3% lower, relative time 0.73, p = 0.01, treatment 160, control 160. | |
| Sarojvisut, 12/12/2022, Randomized Controlled Trial, Thailand, peer-reviewed, 8 authors, study period 1 October, 2021 - 31 May, 2022, dosage 400μg/kg days 1-5, trial TCTR20220427005. | risk of ICU admission, 103.8% higher, RR 2.04, p = 0.62, treatment 2 of 157 (1.3%), control 1 of 160 (0.6%). |
| risk of no improvement, 103.8% higher, RR 2.04, p = 0.62, treatment 2 of 157 (1.3%), control 1 of 160 (0.6%). | |
| recovery time, 3.8% lower, relative time 0.96, p = 0.63, treatment 157, control 160. | |
| Shahbaznejad, 1/19/2021, Double Blind Randomized Controlled Trial, Iran, peer-reviewed, 8 authors, average treatment delay 6.29 days, dosage 200μg/kg single dose, trial IRCT20111224008507N3. | risk of death, 197.1% higher, RR 2.97, p = 1.00, treatment 1 of 35 (2.9%), control 0 of 34 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), patient died within 24 hours of admission. |
| risk of mechanical ventilation, 94.3% higher, RR 1.94, p = 1.00, treatment 2 of 35 (5.7%), control 1 of 34 (2.9%). | |
| recovery time, 31.6% lower, relative time 0.68, p = 0.048, treatment 35, control 34, duration of dsypnea. | |
| recovery time, 19.2% lower, relative time 0.81, p = 0.02, treatment 35, control 34, duration of all symptoms, primary outcome. | |
| hospitalization time, 15.5% lower, relative time 0.85, p = 0.02, treatment 35, control 34. | |
| Shimizu, 12/31/2021, retrospective, Japan, peer-reviewed, 11 authors, study period December 2020 - May 2021, dosage 200μg/kg days 1, 14. | risk of death, 99.9% lower, HR 0.001, p < 0.001, treatment 0 of 39 (0.0%), control 8 of 49 (16.3%), NNT 6.1, adjusted per study, Cox proportional hazard regression. |
| ventilator free days, 47.9% lower, OR 0.52, p = 0.03, treatment 39, control 49, adjusted per study, inverted to make OR<1 favor treatment, proportional odds logistic regression, primary outcome, RR approximated with OR. | |
| ventilation time, 38.5% lower, relative time 0.62, p < 0.001, treatment 39, control 49. | |
| ICU free days, 42.8% lower, OR 0.57, p = 0.06, treatment 39, control 49, adjusted per study, inverted to make OR<1 favor treatment, proportional odds logistic regression, RR approximated with OR. | |
| ICU time, 37.5% lower, relative time 0.62, p < 0.001, treatment 39, control 49. | |
| GI complications while ventilated, 77.9% lower, RR 0.22, p = 0.03, treatment 39, control 49, adjusted per study, Cox proportional hazard regression. | |
| Soto, 3/2/2022, retrospective, Peru, peer-reviewed, median age 58.0, 10 authors, study period April 2020 - August 2020, dosage not specified, excluded in exclusion analyses: substantial unadjusted confounding by indication likely; substantial confounding by time possible due to significant changes in SOC and treatment propensity near the start of the pandemic. | risk of death, 41.0% higher, HR 1.41, p = 0.001, treatment 280 of 484 (57.9%), control 374 of 934 (40.0%), adjusted per study, multivariable. |
| Soto-Becerra, 10/8/2020, retrospective, database analysis, Peru, preprint, median age 59.4, 4 authors, study period 1 April, 2020 - 19 July, 2020, dosage 200μg/kg single dose, excluded in exclusion analyses: substantial unadjusted confounding by indication likely; includes PCR+ patients that may be asymptomatic for COVID-19 but in hospital for other reasons. | risk of death, 17.1% lower, HR 0.83, p = 0.01, treatment 92 of 203 (45.3%), control 1,438 of 2,630 (54.7%), NNT 11, IVM vs. control day 43 (last day available) weighted KM from figure 3, per the pre-specified rules, the last available day mortality results have priority. |
| risk of death, 39.0% higher, HR 1.39, p = 0.16, treatment 47 of 203 (23.2%), control 401 of 2,630 (15.2%), adjusted per study, day 30, Table 2, IVM wHR, primary outcome. | |
| Spoorthi, 11/14/2020, prospective, India, peer-reviewed, 2 authors, dosage not specified, this trial uses multiple treatments in the treatment arm (combined with doxycycline) - results of individual treatments may vary. | recovery time, 21.1% lower, relative time 0.79, p = 0.03, treatment 50, control 50. |
| hospitalization time, 15.5% lower, relative time 0.84, p = 0.01, treatment 50, control 50. | |
| Thairu, 2/25/2022, retrospective, Nigeria, peer-reviewed, mean age 41.7, 6 authors, study period April 2021 - November 2021, dosage 200μg/kg days 1-5, excluded in exclusion analyses: significant confounding by time possible due to separation of groups in different time periods. | risk of death, 87.9% lower, RR 0.12, p = 0.12, treatment 0 of 21 (0.0%), control 4 of 26 (15.4%), NNT 6.5, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), propensity score matching. |
| risk of death, 93.0% lower, RR 0.07, p = 0.007, treatment 0 of 61 (0.0%), control 4 of 26 (15.4%), NNT 6.5, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), all patients. | |
| time to discharge, 54.6% lower, relative time 0.45, p < 0.001, treatment 61, control 26, propensity score matching. | |
| risk of no viral clearance, 94.8% lower, RR 0.05, p = 0.001, treatment 0 of 21 (0.0%), control 10 of 26 (38.5%), NNT 2.6, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), propensity score matching, day 21. | |
| risk of no viral clearance, 95.2% lower, RR 0.05, p < 0.001, treatment 1 of 21 (4.8%), control 26 of 26 (100.0%), NNT 1.1, propensity score matching, day 14. | |
| risk of no viral clearance, 28.6% lower, RR 0.71, p = 0.005, treatment 15 of 21 (71.4%), control 26 of 26 (100.0%), NNT 3.5, propensity score matching, day 5. | |
| Varnaseri, 4/30/2024, Double Blind Randomized Controlled Trial, placebo-controlled, Iran, peer-reviewed, 14 authors, study period July 2020 - June 2021, dosage 14mg bid days 1-3. | risk of mechanical ventilation, 81.8% lower, RR 0.18, p = 0.02, treatment 2 of 55 (3.6%), control 11 of 55 (20.0%), NNT 6.1. |
| risk of ICU admission, 83.3% lower, RR 0.17, p < 0.001, treatment 3 of 55 (5.5%), control 18 of 55 (32.7%), NNT 3.7. | |
| hospitalization time, 33.3% lower, relative time 0.67, p < 0.001, treatment 55, control 55. | |
| recovery time, 28.4% lower, relative time 0.72, p < 0.001, treatment 55, control 55, all symptoms combined. | |
| recovery time, 25.0% lower, relative time 0.75, p < 0.001, treatment 55, control 55, dyspnea. | |
| recovery time, 25.0% lower, relative time 0.75, p < 0.001, treatment 55, control 55, fever. | |
| recovery time, 25.0% lower, relative time 0.75, p < 0.001, treatment 55, control 55, shivering. | |
| recovery time, 40.0% lower, relative time 0.60, p < 0.001, treatment 55, control 55, cough. | |
| recovery time, 37.5% lower, relative time 0.62, p = 0.09, treatment 55, control 55, sore throat. | |
| recovery time, 25.0% lower, relative time 0.75, p = 0.01, treatment 55, control 55, nausea. | |
| recovery time, 37.5% lower, relative time 0.62, p = 0.005, treatment 55, control 55, diarrhea. | |
| recovery time, 40.0% lower, relative time 0.60, p < 0.001, treatment 55, control 55, myalgia. | |
| Wada, 5/22/2023, Double Blind Randomized Controlled Trial, placebo-controlled, Japan, peer-reviewed, 26 authors, study period August 2020 - October 2021, average treatment delay 6.6 days, dosage 200μg/kg single dose, trial NCT04703205 (history). | risk of progression, 19.0% lower, RR 0.81, p = 0.46, treatment 19 of 106 (17.9%), control 23 of 106 (21.7%), NNT 26, adjusted per study, odds ratio converted to relative risk. |
| risk of progression, 27.1% lower, RR 0.73, p = 0.47, treatment 7 of 28 (25.0%), control 9 of 29 (31.0%), NNT 17, adjusted per study, odds ratio converted to relative risk, pneumonia for patients w/o pneumonia at baseline. | |
| risk of oxygen therapy, 14.3% higher, RR 1.14, p = 0.46, treatment 22 of 106 (20.8%), control 19 of 106 (17.9%), adjusted per study, odds ratio converted to relative risk. | |
| improvement, 23.5% worse, OR 1.23, p = 0.61, treatment 106, control 106, adjusted per study, inverted to make OR<1 favor treatment, RR approximated with OR. | |
| risk of no recovery, 60.0% lower, RR 0.40, p = 0.17, treatment 4 of 107 (3.7%), control 10 of 107 (9.3%), NNT 18, day 15, dyspnea. | |
| risk of no recovery, 20.0% lower, RR 0.80, p = 1.00, treatment 4 of 107 (3.7%), control 5 of 107 (4.7%), NNT 107, day 15, headache. | |
| risk of no recovery, no change, RR 1.00, p = 1.00, treatment 7 of 107 (6.5%), control 7 of 107 (6.5%), day 15, sore throat. | |
| risk of no recovery, 18.2% lower, RR 0.82, p = 0.81, treatment 9 of 107 (8.4%), control 11 of 107 (10.3%), NNT 53, day 15, nasal discharge. | |
| risk of no recovery, 3.8% higher, RR 1.04, p = 1.00, treatment 27 of 107 (25.2%), control 26 of 107 (24.3%), day 15, cough. | |
| risk of no recovery, no change, RR 1.00, p = 1.00, treatment 18 of 107 (16.8%), control 18 of 107 (16.8%), day 15, sputum. | |
| risk of no recovery, 20.0% lower, RR 0.80, p = 1.00, treatment 4 of 107 (3.7%), control 5 of 107 (4.7%), NNT 107, day 15, diarhhea. | |
| risk of no recovery, 66.7% higher, RR 1.67, p = 0.72, treatment 5 of 107 (4.7%), control 3 of 107 (2.8%), day 15, myalgia. | |
| risk of no recovery, 1000.0% higher, RR 11.00, p = 0.06, treatment 5 of 107 (4.7%), control 0 of 107 (0.0%), continuity correction due to zero event (with reciprocal of the contrasting arm), day 15, arthralgia. | |
| risk of no viral clearance, 4.2% higher, HR 1.04, p = 0.79, treatment 106, control 106, inverted to make HR<1 favor treatment, Kaplan–Meier, primary outcome. | |
| Zubair, 1/18/2022, retrospective, Pakistan, peer-reviewed, 8 authors, study period October 2020 - February 2021, dosage 12mg single dose, excluded in exclusion analyses: substantial unadjusted confounding by indication likely; unadjusted results with no group details. | risk of death, 9.0% higher, RR 1.09, p = 1.00, treatment 5 of 90 (5.6%), control 5 of 98 (5.1%), unadjusted. |
| hospitalization time, 8.0% higher, relative time 1.08, p = 0.40, treatment 90, control 98, unadjusted, Table 3, mean number of days. |
Effect extraction follows pre-specified rules as detailed above
and gives priority to more serious outcomes. Only the first (most serious)
outcome is used in pooled analysis, which may differ from the effect a paper
focuses on. Other outcomes are used in outcome specific analyses.
| Alam, 12/15/2020, prospective, Bangladesh, peer-reviewed, 13 authors, dosage 12mg monthly. | risk of case, 90.6% lower, RR 0.09, p < 0.001, treatment 4 of 58 (6.9%), control 44 of 60 (73.3%), NNT 1.5. |
| Behera (B), 2/15/2021, prospective, India, peer-reviewed, 14 authors, dosage 300μg/kg days 1, 4. | risk of case, 83.0% lower, RR 0.17, p < 0.001, treatment 45 of 2,199 (2.0%), control 133 of 1,147 (11.6%), NNT 10, two doses, primary outcome. |
| Behera, 11/3/2020, retrospective, India, peer-reviewed, 13 authors, dosage 300μg/kg days 1, 4. | risk of case, 53.8% lower, RR 0.46, p < 0.001, treatment 41 of 117 (35.0%), control 145 of 255 (56.9%), NNT 4.6, adjusted per study, odds ratio converted to relative risk, model 2 2+ doses conditional logistic regression. |
| Bernigaud, 11/28/2020, retrospective, France, peer-reviewed, 12 authors, dosage 200μg/kg days 1, 8, 15, 400μg/kg days 1, 8, 15, two different dosages. | risk of death, 99.4% lower, RR 0.006, p = 0.08, treatment 0 of 69 (0.0%), control 150 of 3,062 (4.9%), NNT 20, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| risk of case, 55.1% lower, RR 0.45, p = 0.01, treatment 7 of 69 (10.1%), control 692 of 3,062 (22.6%), NNT 8.0. | |
| Carvallo, 11/17/2020, prospective, Argentina, peer-reviewed, 4 authors, dosage 12mg weekly, this trial uses multiple treatments in the treatment arm (combined with iota-carrageenan) - results of individual treatments may vary, excluded in exclusion analyses: concern about potential data issues. | risk of case, 99.9% lower, RR 0.001, p < 0.001, treatment 0 of 788 (0.0%), control 237 of 407 (58.2%), NNT 1.7, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| Carvallo (B), 10/19/2020, prospective, Argentina, preprint, 1 author, dosage 1mg days 1-14, this trial uses multiple treatments in the treatment arm (combined with iota-carrageenan) - results of individual treatments may vary, trial NCT04425850 (history), excluded in exclusion analyses: concern about potential data issues. | risk of case, 96.3% lower, RR 0.04, p < 0.001, treatment 0 of 131 (0.0%), control 11 of 98 (11.2%), NNT 8.9, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm). |
| Chahla (B), 1/11/2021, Randomized Controlled Trial, Argentina, peer-reviewed, 11 authors, study period 15 October, 2020 - 31 December, 2020, dosage 12mg weekly, this trial uses multiple treatments in the treatment arm (combined with iota-carrageenan) - results of individual treatments may vary, trial NCT04701710 (history). | risk of moderate/severe case, 95.2% lower, RR 0.05, p = 0.002, treatment 0 of 117 (0.0%), control 10 of 117 (8.5%), NNT 12, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), moderate/severe COVID-19. |
| risk of case, 84.0% lower, RR 0.16, p = 0.004, treatment 4 of 117 (3.4%), control 25 of 117 (21.4%), NNT 5.6, adjusted per study, odds ratio converted to relative risk, all cases, primary outcome. | |
| Desort-Henin, 1/5/2023, Double Blind Randomized Controlled Trial, placebo-controlled, Bulgaria, preprint, 5 authors, study period March 2022 - October 2022, dosage 200μg/kg day 1, 100μg/kg days 2-28, trial NCT05305560 (history) (SAIVE). | risk of case with high viral load, 96.0% lower, RR 0.04, p < 0.001, treatment 4 of 200 (2.0%), control 99 of 199 (49.7%), NNT 2.1. |
| risk of case, 71.6% lower, RR 0.28, p < 0.001, treatment 30 of 200 (15.0%), control 105 of 199 (52.8%), NNT 2.6, primary outcome. | |
| Hellwig, 11/28/2020, retrospective, ecological study, multiple countries, peer-reviewed, 2 authors, dosage 200μg/kg, dose varied, typically 150-200μg/kg, excluded in exclusion analyses: not a typical trial, analysis of African countries that used or did not use ivermectin prophylaxis for parasitic infections. | risk of case, 78.0% lower, RR 0.22, p < 0.02, African countries, PCTI vs. no PCT, relative cases per capita. |
| IVERCOR PREP, 12/20/2020, retrospective, Argentina, preprint, 1 author, dosage 12mg weekly, excluded in exclusion analyses: minimal details provided. | risk of case, 73.4% lower, RR 0.27, p < 0.001, treatment 13 of 389 (3.3%), control 61 of 486 (12.6%), NNT 11. |
| Kerr, 12/11/2021, retrospective, propensity score matching, Brazil, peer-reviewed, 9 authors, study period July 2020 - December 2020, dosage 200μg/kg days 1, 2, 16, 17, 0.2mg/kg/day for 2 days every 15 days. | risk of death, 70.0% lower, RR 0.30, p < 0.001, treatment 25 of 3,034 (0.8%), control 79 of 3,034 (2.6%), NNT 56, adjusted per study, multivariate linear regression, propensity score matching. |
| risk of hospitalization, 67.0% lower, RR 0.33, p < 0.001, treatment 44 of 3,034 (1.5%), control 99 of 3,034 (3.3%), adjusted per study, multivariate linear regression, propensity score matching. | |
| risk of case, 44.5% lower, RR 0.56, p < 0.001, treatment 4,197 of 113,845 (3.7%), control 3,034 of 45,716 (6.6%), NNT 34. | |
| Mondal, 5/31/2021, retrospective, India, peer-reviewed, 11 authors, dosage not specified. | risk of symptomatic case, 87.9% lower, RR 0.12, p = 0.006, treatment 128, control 1,342, adjusted per study, odds ratio converted to relative risk, control prevalence approximated with overall prevalence, multivariable, primary outcome. | Moraes, 4/30/2021, Randomized Controlled Trial, this trial compares with another treatment - results may be better when compared to placebo, trial NCT04384458 (history). | Estimated 400 patient RCT with results unknown and over 4 years late. |
| Morgenstern, 4/16/2021, retrospective, propensity score matching, Dominican Republic, peer-reviewed, 16 authors, dosage 200μg/kg weekly, trial NCT04832945 (history). | risk of hospitalization, 80.0% lower, RR 0.20, p = 0.50, treatment 0 of 271 (0.0%), control 2 of 271 (0.7%), NNT 136, relative risk is not 0 because of continuity correction due to zero events (with reciprocal of the contrasting arm), PSM. |
| risk of case, 74.0% lower, RR 0.26, p = 0.008, treatment 5 of 271 (1.8%), control 18 of 271 (6.6%), NNT 21, adjusted per study, PSM, multivariate Cox regression, primary outcome. | PREVENT-COVID, 6/24/2023, Double Blind Randomized Controlled Trial, placebo-controlled, trial NCT05060666 (history) (PREVENT-COVID). | Estimated 412 patient RCT with results unknown and over 3 years late. |
| Samajdar, 11/17/2021, retrospective, India, peer-reviewed, 9 authors, study period 1 September, 2020 - 31 December, 2020, dosage not specified, excluded in exclusion analyses: minimal details provided; unadjusted results with no group details; results may be significantly affected by survey bias. | risk of case, 79.8% lower, RR 0.20, p < 0.001, treatment 12 of 164 (7.3%), control 29 of 81 (35.8%), NNT 3.5, odds ratio converted to relative risk, physician survey. |
| risk of case, 48.6% lower, RR 0.51, p = 0.03, treatment 11 of 109 (10.1%), control 39 of 200 (19.5%), NNT 11, odds ratio converted to relative risk, combined ivermectin or HCQ in community. | |
| Seet, 4/14/2021, Cluster Randomized Controlled Trial, Singapore, peer-reviewed, 15 authors, study period 13 May, 2020 - 31 August, 2020, dosage 12mg single dose, 200µg/kg, maximum 12mg, this trial compares with another treatment - results may be better when compared to placebo, trial NCT04446104 (history). | risk of symptomatic case, 49.8% lower, RR 0.50, p < 0.001, treatment 32 of 617 (5.2%), control 64 of 619 (10.3%), NNT 19. |
| risk of case, 5.8% lower, RR 0.94, p = 0.61, treatment 398 of 617 (64.5%), control 433 of 619 (70.0%), NNT 18, adjusted per study, odds ratio converted to relative risk, model 6, primary outcome. | |
| Shouman (B), 8/28/2020, Randomized Controlled Trial, Egypt, peer-reviewed, 8 authors, study period 1 June, 2020 - 28 July, 2020, dosage 18mg days 1, 3, dose varies depending on weight - 40-60kg: 15mg, 60-80kg: 18mg, >80kg: 24mg, trial NCT04422561 (history). | risk of symptomatic case, 91.3% lower, RR 0.09, p < 0.001, treatment 15 of 203 (7.4%), control 59 of 101 (58.4%), NNT 2.0, adjusted per study, inverted to make RR<1 favor treatment, multivariate, primary outcome. |
| risk of severe case, 92.9% lower, RR 0.07, p = 0.002, treatment 1 of 203 (0.5%), control 7 of 101 (6.9%), NNT 16, unadjusted. | |
| Tanioka, 3/26/2021, retrospective, ecological study, multiple countries, preprint, 3 authors, dosage 200μg/kg, dose varied, typically 150-200μg/kg, excluded in exclusion analyses: not a typical trial, analysis of African countries that used or did not use ivermectin prophylaxis for parasitic infections. | risk of death, 88.2% lower, RR 0.12, p = 0.002, relative mean mortality per million. |
Viral infection and replication involves attachment, entry, uncoating and release, genome replication and transcription, translation and protein processing, assembly and budding, and release. Each step can be disrupted by therapeutics.
Guzzo et al., Safety, Tolerability, and Pharmacokinetics of Escalating High Doses of Ivermectin in Healthy Adult Subjects, J. Clinical Pharmacology, doi:10.1177/009127002237994.
Williams, T., Not All Ivermectin Is Created Equal: Comparing The Quality of 11 Different Ivermectin Sources, Do Your Own Research, doyourownresearch.substack.com/p/not-all-ivermectin-is-created-equal.
Kory et al., Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19, American Journal of Therapeutics, doi:10.1097/MJT.0000000000001377.
Lawrie et al., Ivermectin reduces the risk of death from COVID-19 – a rapid review and meta-analysis in support of the recommendation of the Front Line COVID-19 Critical Care Alliance, Preprint, b3d2650e-e929-4448-a527-4eeb59304c7f.filesusr.com/ugd/593c4f_8cb655bd21b1448ba6cf1f4c59f0d73d.pdf.
Bryant et al., Ivermectin for Prevention and Treatment of COVID-19 Infection: A Systematic Review, Meta-analysis, and Trial Sequential Analysis to Inform Clinical Guidelines, American Journal of Therapeutics, doi:10.1097/MJT.0000000000001402.
Nardelli et al., Crying wolf in time of Corona: the strange case of ivermectin and hydroxychloroquine. Is the fear of failure withholding potential life-saving treatment from clinical use?, Signa Vitae, doi:10.22514/sv.2021.043.
Hariyanto et al., Ivermectin and outcomes from Covid-19 pneumonia: A systematic review and meta-analysis of randomized clinical trial studies, Reviews In Medical Virology, doi:10.1002/rmv.2265.
Ryu et al., Fibrin drives thromboinflammation and neuropathology in COVID-19, Nature, doi:10.1038/s41586-024-07873-4.
Rong et al., Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19, Cell Host & Microbe, doi:10.1016/j.chom.2024.11.007.
Yang et al., SARS-CoV-2 infection causes dopaminergic neuron senescence, Cell Stem Cell, doi:10.1016/j.stem.2023.12.012.
Scardua-Silva et al., Microstructural brain abnormalities, fatigue, and cognitive dysfunction after mild COVID-19, Scientific Reports, doi:10.1038/s41598-024-52005-7.
Hampshire et al., Cognition and Memory after Covid-19 in a Large Community Sample, New England Journal of Medicine, doi:10.1056/NEJMoa2311330.
Duloquin et al., Is COVID-19 Infection a Multiorganic Disease? Focus on Extrapulmonary Involvement of SARS-CoV-2, Journal of Clinical Medicine, doi:10.3390/jcm13051397.
Sodagar et al., Pathological Features and Neuroinflammatory Mechanisms of SARS-CoV-2 in the Brain and Potential Therapeutic Approaches, Biomolecules, doi:10.3390/biom12070971.
Sagar et al., COVID-19-associated cerebral microbleeds in the general population, Brain Communications, doi:10.1093/braincomms/fcae127.
Verma et al., Persistent Neurological Deficits in Mouse PASC Reveal Antiviral Drug Limitations, bioRxiv, doi:10.1101/2024.06.02.596989.
Panagea et al., Neurocognitive Impairment in Long COVID: A Systematic Review, Archives of Clinical Neuropsychology, doi:10.1093/arclin/acae042.
Ariza et al., COVID-19: Unveiling the Neuropsychiatric Maze—From Acute to Long-Term Manifestations, Biomedicines, doi:10.3390/biomedicines12061147.
Vashisht et al., Neurological Complications of COVID-19: Unraveling the Pathophysiological Underpinnings and Therapeutic Implications, Viruses, doi:10.3390/v16081183.
Ahmad et al., Neurological Complications and Outcomes in Critically Ill Patients With COVID-19: Results From International Neurological Study Group From the COVID-19 Critical Care Consortium, The Neurohospitalist, doi:10.1177/19418744241292487.
Wang et al., SARS-CoV-2 membrane protein induces neurodegeneration via affecting Golgi-mitochondria interaction, Translational Neurodegeneration, doi:10.1186/s40035-024-00458-1.
Eberhardt et al., SARS-CoV-2 infection triggers pro-atherogenic inflammatory responses in human coronary vessels, Nature Cardiovascular Research, doi:10.1038/s44161-023-00336-5.
Van Tin et al., Spike Protein of SARS-CoV-2 Activates Cardiac Fibrogenesis through NLRP3 Inflammasomes and NF-κB Signaling, Cells, doi:10.3390/cells13161331.
Borka Balas et al., COVID-19 and Cardiac Implications—Still a Mystery in Clinical Practice, Reviews in Cardiovascular Medicine, doi:10.31083/j.rcm2405125.
AlTaweel et al., An In-Depth Insight into Clinical, Cellular and Molecular Factors in COVID19-Associated Cardiovascular Ailments for Identifying Novel Disease Biomarkers, Drug Targets and Clinical Management Strategies, Archives of Microbiology & Immunology, doi:10.26502/ami.936500177.
Saha et al., COVID-19 beyond the lungs: Unraveling its vascular impact and cardiovascular complications—mechanisms and therapeutic implications, Science Progress, doi:10.1177/00368504251322069.
Trender et al., Changes in memory and cognition during the SARS-CoV-2 human challenge study, eClinicalMedicine, doi:10.1016/j.eclinm.2024.102842.
Dugied et al., Multimodal SARS-CoV-2 interactome sketches the virus-host spatial organization, Communications Biology, doi:10.1038/s42003-025-07933-z.
Malone et al., Structures and functions of coronavirus replication–transcription complexes and their relevance for SARS-CoV-2 drug design, Nature Reviews Molecular Cell Biology, doi:10.1038/s41580-021-00432-z.
Murigneux et al., Proteomic analysis of SARS-CoV-2 particles unveils a key role of G3BP proteins in viral assembly, Nature Communications, doi:10.1038/s41467-024-44958-0.
Lv et al., Host proviral and antiviral factors for SARS-CoV-2, Virus Genes, doi:10.1007/s11262-021-01869-2.
Lui et al., Nsp1 facilitates SARS-CoV-2 replication through calcineurin-NFAT signaling, Virology, doi:10.1128/mbio.00392-24.
Niarakis et al., Drug-target identification in COVID-19 disease mechanisms using computational systems biology approaches, Frontiers in Immunology, doi:10.3389/fimmu.2023.1282859.
Katiyar et al., SARS-CoV-2 Assembly: Gaining Infectivity and Beyond, Viruses, doi:10.3390/v16111648.
Wu et al., Decoding the genome of SARS-CoV-2: a pathway to drug development through translation inhibition, RNA Biology, doi:10.1080/15476286.2024.2433830.
Götz et al., Influenza A viruses escape from MxA restriction at the expense of efficient nuclear vRNP import, Scientific Reports, doi:10.1038/srep23138.
Tay et al., Nuclear localization of dengue virus (DENV) 1–4 non-structural protein 5; protection against all 4 DENV serotypes by the inhibitor Ivermectin, Antiviral Research, doi:10.1016/j.antiviral.2013.06.002.
Wagstaff et al., Ivermectin is a specific inhibitor of importin α/β-mediated nuclear import able to inhibit replication of HIV-1 and dengue virus, Biochemical Journal, doi:10.1042/BJ20120150.
Jitobaom et al., Identification of inositol monophosphatase as a broad‐spectrum antiviral target of ivermectin, Journal of Medical Virology, doi:10.1002/jmv.29552.
Wagstaff (B) et al., An AlphaScreen®-Based Assay for High-Throughput Screening for Specific Inhibitors of Nuclear Import, SLAS Discovery, doi:10.1177/1087057110390360.
Barrows et al., A Screen of FDA-Approved Drugs for Inhibitors of Zika Virus Infection, Cell Host & Microbe, doi:10.1016/j.chom.2016.07.004.
Yang (B) et al., The broad spectrum antiviral ivermectin targets the host nuclear transport importin α/β1 heterodimer, Antiviral Research, doi:10.1016/j.antiviral.2020.104760.
Mastrangelo et al., Ivermectin is a potent inhibitor of flavivirus replication specifically targeting NS3 helicase activity: new prospects for an old drug, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dks147.
Varghese et al., Discovery of berberine, abamectin and ivermectin as antivirals against chikungunya and other alphaviruses, Antiviral Research, doi:10.1016/j.antiviral.2015.12.012.
Li et al., Quantitative proteomics reveals a broad-spectrum antiviral property of ivermectin, benefiting for COVID-19 treatment, J. Cellular Physiology, doi:10.1002/jcp.30055.
Bennett et al., Role of a nuclear localization signal on the minor capsid Proteins VP2 and VP3 in BKPyV nuclear entry, Virology, doi:10.1016/j.virol.2014.10.013.
Kosyna et al., The importin α/β-specific inhibitor Ivermectin affects HIF-dependent hypoxia response pathways, Biological Chemistry, doi:10.1515/hsz-2015-0171.
Fauquet et al., Microfluidic Diffusion Sizing Applied to the Study of Natural Products and Extracts That Modulate the SARS-CoV-2 Spike RBD/ACE2 Interaction, Molecules, doi:10.3390/molecules28248072.
Boschi et al., SARS-CoV-2 Spike Protein Induces Hemagglutination: Implications for COVID-19 Morbidities and Therapeutics and for Vaccine Adverse Effects, bioRxiv, doi:10.1101/2022.11.24.517882.
Scheim et al., Sialylated Glycan Bindings from SARS-CoV-2 Spike Protein to Blood and Endothelial Cells Govern the Severe Morbidities of COVID-19, International Journal of Molecular Sciences, doi:10.3390/ijms242317039.
Shahin et al., The selective effect of Ivermectin on different human coronaviruses; in-vitro study, Research Square, doi:10.21203/rs.3.rs-4180797/v1.
Abd-Elmawla et al., Suppression of NLRP3 inflammasome by ivermectin ameliorates bleomycin-induced pulmonary fibrosis, Journal of Zhejiang University-SCIENCE B, doi:10.1631/jzus.B2200385.
Ma et al., Ivermectin contributes to attenuating the severity of acute lung injury in mice, Biomedicine & Pharmacotherapy, doi:10.1016/j.biopha.2022.113706.
Vottero et al., Computational Prediction of the Interaction of Ivermectin with Fibrinogen, Molecular Sciences, doi:10.3390/ijms241411449.
Mody et al., Identification of 3-chymotrypsin like protease (3CLPro) inhibitors as potential anti-SARS-CoV-2 agents, Communications Biology, doi:10.1038/s42003-020-01577-x.
Parvez et al., Prediction of potential inhibitors for RNA-dependent RNA polymerase of SARS-CoV-2 using comprehensive drug repurposing and molecular docking approach, International Journal of Biological Macromolecules, doi:10.1016/j.ijbiomac.2020.09.098.
Gao et al., Ivermectin ameliorates acute myocarditis via the inhibition of importin-mediated nuclear translocation of NF-κB/p65, International Immunopharmacology, doi:10.1016/j.intimp.2024.112073.
Liu et al., Crosstalk between neutrophil extracellular traps and immune regulation: insights into pathobiology and therapeutic implications of transfusion-related acute lung injury, Frontiers in Immunology, doi:10.3389/fimmu.2023.1324021.
Bagheri-Far et al., Non-spike protein inhibition of SARS-CoV-2 by natural products through the key mediator protein ORF8, Molecular Biology Research Communications, doi:10.22099/mbrc.2024.50245.2001.
Shouman et al., SARS-CoV-2-associated lymphopenia: possible mechanisms and the role of CD147, Cell Communication and Signaling, doi:10.1186/s12964-024-01718-3.
Scheim (B), D., Ivermectin for COVID-19 Treatment: Clinical Response at Quasi-Threshold Doses Via Hypothesized Alleviation of CD147-Mediated Vascular Occlusion, SSRN, doi:10.2139/ssrn.3636557.
Scheim (C), D., From Cold to Killer: How SARS-CoV-2 Evolved without Hemagglutinin Esterase to Agglutinate and Then Clot Blood Cells, Center for Open Science, doi:10.31219/osf.io/sgdj2.
Behl et al., CD147-spike protein interaction in COVID-19: Get the ball rolling with a novel receptor and therapeutic target, Science of The Total Environment, doi:10.1016/j.scitotenv.2021.152072.
Zhang et al., Ivermectin inhibits LPS-induced production of inflammatory cytokines and improves LPS-induced survival in mice, Inflammation Research, doi:10.1007/s00011-008-8007-8.
DiNicolantonio et al., Ivermectin may be a clinically useful anti-inflammatory agent for late-stage COVID-19, Open Heart, doi:10.1136/openhrt-2020-001350.
Zhao et al., Identification of the shared gene signatures between pulmonary fibrosis and pulmonary hypertension using bioinformatics analysis, Frontiers in Immunology, doi:10.3389/fimmu.2023.1197752.
Liu (B) et al., Genome-wide analyses reveal the detrimental impacts of SARS-CoV-2 viral gene Orf9c on human pluripotent stem cell-derived cardiomyocytes, Stem Cell Reports, doi:10.1016/j.stemcr.2022.01.014.
Liu (C) et al., SARS-CoV-2 viral genes Nsp6, Nsp8, and M compromise cellular ATP levels to impair survival and function of human pluripotent stem cell-derived cardiomyocytes, Stem Cell Research & Therapy, doi:10.1186/s13287-023-03485-3.
Mothae et al., SARS-CoV-2 host-pathogen interactome: insights into more players during pathogenesis, Virology, doi:10.1016/j.virol.2025.110607.
Gayozo et al., Binding affinities analysis of ivermectin, nucleocapsid and ORF6 proteins of SARS-CoV-2 to human importins α isoforms: A computational approach, Biotecnia, doi:10.18633/biotecnia.v27.2485.
Kofler et al., M-Motif, a potential non-conventional NLS in YAP/TAZ and other cellular and viral proteins that inhibits classic protein import, iScience, doi:10.1016/j.isci.2025.112105.
Hazan et al., Treatment with Ivermectin Increases the Population of Bifidobacterium in the Gut, ACG 2023, acg2023posters.eventscribe.net/posterspeakers.asp.
Munson et al., Niclosamide and ivermectin modulate caspase-1 activity and proinflammatory cytokine secretion in a monocytic cell line, British Society For Nanomedicine Early Career Researcher Summer Meeting, 2021, web.archive.org/web/20230401070026/https://michealmunson.github.io/COVID.pdf.
DiNicolantonio (B) et al., Anti-inflammatory activity of ivermectin in late-stage COVID-19 may reflect activation of systemic glycine receptors, Open Heart, doi:10.1136/openhrt-2021-001655.
Yan et al., Anti-inflammatory effects of ivermectin in mouse model of allergic asthma, Inflammation Research, doi:10.1007/s00011-011-0307-8.
Descotes, J., Medical Safety of Ivermectin, ImmunoSafe Consultance, web.archive.org/web/20240313025927/https://www.medincell.com/wp-content/uploads/2021/03/Clinical_Safety_of_Ivermectin-March_2021.pdf.
Lefebvre et al., Characterization and Fluctuations of an Ivermectin Binding Site at the Lipid Raft Interface of the N-Terminal Domain (NTD) of the Spike Protein of SARS-CoV-2 Variants, Viruses, doi:10.3390/v16121836.
Haque et al., Exploring potential therapeutic candidates against COVID-19: a molecular docking study, Discover Molecules, doi:10.1007/s44345-024-00005-5.
de Oliveira Só et al., In Silico Comparative Analysis of Ivermectin and Nirmatrelvir Inhibitors Interacting with the SARS-CoV-2 Main Protease, Preprints, doi:10.20944/preprints202404.1825.v1.
Agamah et al., Network-based multi-omics-disease-drug associations reveal drug repurposing candidates for COVID-19 disease phases, ScienceOpen, doi:10.58647/DRUGARXIV.PR000010.v1.
Oranu et al., Validation of the binding affinities and stabilities of ivermectin and moxidectin against SARS-CoV-2 receptors using molecular docking and molecular dynamics simulation, GSC Biological and Pharmaceutical Sciences, doi:10.30574/gscbps.2024.26.1.0030.
Chellasamy et al., Docking and molecular dynamics studies of human ezrin protein with a modelled SARS-CoV-2 endodomain and their interaction with potential invasion inhibitors, Journal of King Saud University - Science, doi:10.1016/j.jksus.2022.102277.
Umar et al., Inhibitory potentials of ivermectin, nafamostat, and camostat on spike protein and some nonstructural proteins of SARS-CoV-2: Virtual screening approach, Jurnal Teknologi Laboratorium, doi:10.29238/teknolabjournal.v11i1.344.
Alvarado et al., Interaction of the New Inhibitor Paxlovid (PF-07321332) and Ivermectin With the Monomer of the Main Protease SARS-CoV-2: A Volumetric Study Based on Molecular Dynamics, Elastic Networks, Classical Thermodynamics and SPT, Computational Biology and Chemistry, doi:10.1016/j.compbiolchem.2022.107692.
Aminpour et al., In Silico Analysis of the Multi-Targeted Mode of Action of Ivermectin and Related Compounds, Computation, doi:10.3390/computation10040051.
Parvez (B) et al., Insights from a computational analysis of the SARS-CoV-2 Omicron variant: Host–pathogen interaction, pathogenicity, and possible drug therapeutics, Immunity, Inflammation and Disease, doi:10.1002/iid3.639.
Francés-Monerris et al., Microscopic interactions between ivermectin and key human and viral proteins involved in SARS-CoV-2 infection, Physical Chemistry Chemical Physics, doi:10.1039/D1CP02967C.
González-Paz et al., Comparative study of the interaction of ivermectin with proteins of interest associated with SARS-CoV-2: A computational and biophysical approach, Biophysical Chemistry, doi:10.1016/j.bpc.2021.106677.
González-Paz (B) et al., Structural Deformability Induced in Proteins of Potential Interest Associated with COVID-19 by binding of Homologues present in Ivermectin: Comparative Study Based in Elastic Networks Models, Journal of Molecular Liquids, doi:10.1016/j.molliq.2021.117284.
Rana et al., A Computational Study of Ivermectin and Doxycycline Combination Drug Against SARS-CoV-2 Infection, Research Square, doi:10.21203/rs.3.rs-755838/v1.
Muthusamy et al., Virtual Screening Reveals Potential Anti-Parasitic Drugs Inhibiting the Receptor Binding Domain of SARS-CoV-2 Spike protein, Journal of Virology & Antiviral Research, www.scitechnol.com/abstract/virtual-screening-reveals-potential-antiparasitic-drugs-inhibiting-the-receptor-binding-domain-of-sarscov2-spike-protein-16398.html.
Qureshi et al., Mechanistic insights into the inhibitory activity of FDA approved ivermectin against SARS-CoV-2: old drug with new implications, Journal of Biomolecular Structure and Dynamics, doi:10.1080/07391102.2021.1906750.
Schöning et al., Highly-transmissible Variants of SARS-CoV-2 May Be More Susceptible to Drug Therapy Than Wild Type Strains, Research Square, doi:10.21203/rs.3.rs-379291/v1.
Bello et al., Elucidation of the inhibitory activity of ivermectin with host nuclear importin α and several SARS-CoV-2 targets, Journal of Biomolecular Structure and Dynamics, doi:10.1080/07391102.2021.1911857.
Udofia et al., In silico studies of selected multi-drug targeting against 3CLpro and nsp12 RNA-dependent RNA-polymerase proteins of SARS-CoV-2 and SARS-CoV, Network Modeling Analysis in Health Informatics and Bioinformatics, doi:10.1007/s13721-021-00299-2.
Choudhury et al., Exploring the binding efficacy of ivermectin against the key proteins of SARS-CoV-2 pathogenesis: an in silico approach, Future Medicine, doi:10.2217/fvl-2020-0342.
Kern et al., Modeling of SARS-CoV-2 Treatment Effects for Informed Drug Repurposing, Frontiers in Pharmacology, doi:10.3389/fphar.2021.625678.
Saha (B) et al., The Binding mechanism of ivermectin and levosalbutamol with spike protein of SARS-CoV-2, Structural Chemistry, doi:10.1007/s11224-021-01776-0.
Eweas et al., Molecular Docking Reveals Ivermectin and Remdesivir as Potential Repurposed Drugs Against SARS-CoV-2, Frontiers in Microbiology, doi:10.3389/fmicb.2020.592908.
Francés-Monerris (B) et al., Has Ivermectin Virus-Directed Effects against SARS-CoV-2? Rationalizing the Action of a Potential Multitarget Antiviral Agent, ChemRxiv, doi:10.26434/chemrxiv.12782258.v1.
Kalhor et al., Repurposing of the approved small molecule drugs in order to inhibit SARS-CoV-2 S protein and human ACE2 interaction through virtual screening approaches, Journal of Biomolecular Structure and Dynamics, doi:10.1080/07391102.2020.1824816.
Swargiary, A., Ivermectin as a promising RNA-dependent RNA polymerase inhibitor and a therapeutic drug against SARS-CoV2: Evidence from in silico studies, Research Square, doi:10.21203/rs.3.rs-73308/v1.
Maurya, D., A Combination of Ivermectin and Doxycycline Possibly Blocks the Viral Entry and Modulate the Innate Immune Response in COVID-19 Patients, American Chemical Society (ACS), doi:10.26434/chemrxiv.12630539.v1.
Lehrer et al., Ivermectin Docks to the SARS-CoV-2 Spike Receptor-binding Domain Attached to ACE2, In Vivo, 34:5, 3023-3026, doi:10.21873/invivo.12134.
Suravajhala et al., Comparative Docking Studies on Curcumin with COVID-19 Proteins, Preprints, doi:10.20944/preprints202005.0439.v3.
García-Aguilar et al., In Vitro Analysis of SARS-CoV-2 Spike Protein and Ivermectin Interaction, International Journal of Molecular Sciences, doi:10.3390/ijms242216392.
De Forni et al., Synergistic drug combinations designed to fully suppress SARS-CoV-2 in the lung of COVID-19 patients, PLoS ONE, doi:10.1371/journal.pone.0276751.
Saha (C) et al., Manipulation of Spray-Drying Conditions to Develop an Inhalable Ivermectin Dry Powder, Pharmaceutics, doi:10.3390/pharmaceutics14071432.
Jitobaom (B) et al., Synergistic anti-SARS-CoV-2 activity of repurposed anti-parasitic drug combinations, BMC Pharmacology and Toxicology, doi:10.1186/s40360-022-00580-8.
Croci et al., Liposomal Systems as Nanocarriers for the Antiviral Agent Ivermectin, International Journal of Biomaterials, doi:10.1155/2016/8043983.
Zheng et al., Red blood cell-hitchhiking mediated pulmonary delivery of ivermectin: Effects of nanoparticle properties, International Journal of Pharmaceutics, doi:10.1016/j.ijpharm.2022.121719.
Delandre et al., Antiviral Activity of Repurposing Ivermectin against a Panel of 30 Clinical SARS-CoV-2 Strains Belonging to 14 Variants, Pharmaceuticals, doi:10.3390/ph15040445.
Segatori et al., Effect of Ivermectin and Atorvastatin on Nuclear Localization of Importin Alpha and Drug Target Expression Profiling in Host Cells from Nasopharyngeal Swabs of SARS-CoV-2- Positive Patients, Viruses, doi:10.3390/v13102084.
Jitobaom (C) et al., Favipiravir and Ivermectin Showed in Vitro Synergistic Antiviral Activity against SARS-CoV-2, Research Square, doi:10.21203/rs.3.rs-941811/v1.
Mountain Valley MD, Mountain Valley MD Receives Successful Results From BSL-4 COVID-19 Clearance Trial on Three Variants Tested With Ivectosol™, www.globenewswire.com/en/news-release/2021/05/18/2231755/0/en/Mountain-Valley-MD-Receives-Successful-Results-From-BSL-4-COVID-19-Clearance-Trial-on-Three-Variants-Tested-With-Ivectosol.html.
Yesilbag et al., Ivermectin also inhibits the replication of bovine respiratory viruses (BRSV, BPIV-3, BoHV-1, BCoV and BVDV) in vitro, Virus Research, doi:10.1016/j.virusres.2021.198384.
Jeffreys et al., Remdesivir-ivermectin combination displays synergistic interaction with improved in vitro activity against SARS-CoV-2, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2022.106542.
Surnar et al., Clinically Approved Antiviral Drug in an Orally Administrable Nanoparticle for COVID-19, ACS Pharmacol. Transl. Sci., doi:10.1021/acsptsci.0c00179.
Caly et al., The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro, Antiviral Research, doi:10.1016/j.antiviral.2020.104787.
Uematsu et al., Prophylactic administration of ivermectin attenuates SARS-CoV-2 induced disease in a Syrian Hamster Model, The Journal of Antibiotics, doi:10.1038/s41429-023-00623-0.
Albariqi et al., Pharmacokinetics and Safety of Inhaled Ivermectin in Mice as a Potential COVID-19 Treatment, International Journal of Pharmaceutics, doi:10.1016/j.ijpharm.2022.121688.
Errecalde et al., Safety and Pharmacokinetic Assessments of a Novel Ivermectin Nasal Spray Formulation in a Pig Model, Journal of Pharmaceutical Sciences, doi:10.1016/j.xphs.2021.01.017.
Madrid et al., Safety of oral administration of high doses of ivermectin by means of biocompatible polyelectrolytes formulation, Heliyon, doi:10.1016/j.heliyon.2020.e05820.
de Melo et al., Attenuation of clinical and immunological outcomes during SARS-CoV-2 infection by ivermectin, EMBO Mol. Med., doi:10.15252/emmm.202114122.
Arévalo et al., Ivermectin reduces in vivo coronavirus infection in a mouse experimental model, Scientific Reports, doi:10.1038/s41598-021-86679-0.
Chaccour et al., Nebulized ivermectin for COVID-19 and other respiratory diseases, a proof of concept, dose-ranging study in rats, Scientific Reports, doi:10.1038/s41598-020-74084-y.
Mohammed et al., A remodeled ivermectin polycaprolactone-based nanoparticles for inhalation as a promising treatment of pulmonary inflammatory diseases, European Journal of Pharmaceutical Sciences, doi:10.1016/j.ejps.2024.106714.
Albariqi (B) et al., Preparation and Characterization of Inhalable Ivermectin Powders as a Potential COVID-19 Therapy, Journal of Aerosol Medicine and Pulmonary Drug Delivery, doi:10.1089/jamp.2021.0059.
Mansour et al., Safety of inhaled ivermectin as a repurposed direct drug for treatment of COVID-19: A preclinical tolerance study, International Immunopharmacology, doi:10.1016/j.intimp.2021.108004.
Zeraatkar et al., Consistency of covid-19 trial preprints with published reports and impact for decision making: retrospective review, BMJ Medicine, doi:10.1136/bmjmed-2022-0003091.
Davidson et al., No evidence of important difference in summary treatment effects between COVID-19 preprints and peer-reviewed publications: a meta-epidemiological study, Journal of Clinical Epidemiology, doi:10.1016/j.jclinepi.2023.08.011.
Jadad et al., Randomized Controlled Trials: Questions, Answers, and Musings, Second Edition, doi:10.1002/9780470691922.
Gøtzsche, P., Bias in double-blind trials, Doctoral Thesis, University of Copenhagen, www.scientificfreedom.dk/2023/05/16/bias-in-double-blind-trials-doctoral-thesis/.
Als-Nielsen et al., Association of Funding and Conclusions in Randomized Drug Trials, JAMA, doi:10.1001/jama.290.7.921.
Anglemyer et al., Healthcare outcomes assessed with observational study designs compared with those assessed in randomized trials, Cochrane Database of Systematic Reviews 2014, Issue 4, doi:10.1002/14651858.MR000034.pub2.
Lee et al., Analysis of Overall Level of Evidence Behind Infectious Diseases Society of America Practice Guidelines, Arch Intern Med., 2011, 171:1, 18-22, doi:10.1001/archinternmed.2010.482.
Deaton et al., Understanding and misunderstanding randomized controlled trials, Social Science & Medicine, 210, doi:10.1016/j.socscimed.2017.12.005.
Nichol et al., Challenging issues in randomised controlled trials, Injury, 2010, doi: 10.1016/j.injury.2010.03.033, www.injuryjournal.com/article/S0020-1383(10)00233-0/fulltext.
Reis et al., Effect of Early Treatment with Ivermectin among Patients with Covid-19, New England Journal of Medicine, doi:10.1056/NEJMoa2115869.
Naggie et al., Effect of Ivermectin vs Placebo on Time to Sustained Recovery in Outpatients With Mild to Moderate COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2022.18590.
Bramante et al., Randomized Trial of Metformin, Ivermectin, and Fluvoxamine for Covid-19, NEJM, doi:10.1056/NEJMoa2201662.
Hayward et al., Ivermectin for COVID-19 in adults in the community (PRINCIPLE): an open, randomised, controlled, adaptive platform trial of short- and longer-term outcomes, Journal of Infection, doi:10.1016/j.jinf.2024.106130.
López-Medina et al., Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2021.3071.
Vallejos et al., Ivermectin to prevent hospitalizations in patients with COVID-19 (IVERCOR-COVID19) a randomized, double-blind, placebo-controlled trial, BMC Infectious Diseases, doi:10.1186/s12879-021-06348-5.
Beltran Gonzalez et al., Efficacy and Safety of Ivermectin and Hydroxychloroquine in Patients with Severe COVID-19: A Randomized Controlled Trial, Infectious Disease Reports, doi:10.3390/idr14020020.
Soto-Becerra et al., Real-World Effectiveness of hydroxychloroquine, azithromycin, and ivermectin among hospitalized COVID-19 patients: Results of a target trial emulation using observational data from a nationwide Healthcare System in Peru, medRxiv, doi:10.1101/2020.10.06.20208066.
Yim, P., Systemic unreported protocol violations in key ivermectin study, TrialSiteNews, trialsitenews.com/systemic-unreported-protocol-violations-in-key-ivermectin-study/.
IVERCOR PREP, Ivermectina en agentes de salud e IVERCOR COVID19, Preliminary Results, web.archive.org/web/20210226215453/https://twitter.com/Covid19Crusher/status/1365420061859717124.
Hellwig et al., A COVID-19 Prophylaxis? Lower incidence associated with prophylactic administration of Ivermectin, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2020.106248.
Tanioka et al., Why COVID-19 is not so spread in Africa: How does Ivermectin affect it?, medRxiv, doi:10.1101/2021.03.26.21254377.
Shahbaznejad et al., Effects of Ivermectin in Patients With COVID-19: A Multicenter, Double-blind, Randomized, Controlled Clinical Trial, Clinical Therapeutics, doi:10.1016/j.clinthera.2021.04.007.
Galan et al., Phase 2 randomized study on chloroquine, hydroxychloroquine or ivermectin in hospitalized patients with severe manifestations of SARS-CoV-2 infection, Pathogens and Global Health, doi:10.1080/20477724.2021.1890887.
Baqui et al., Ethnic and regional variations in hospital mortality from COVID-19 in Brazil: a cross-sectional observational study, The Lancet Global Health, doi:10.1016/S2214-109X(20)30285-0.
Kishoria et al., Ivermectin as adjuvant to hydroxychloroquine in patients resistant to standard treatment for SARS-CoV-2: results of an open-label randomized clinical study, Paripex - Indian Journal of Research, doi:10.36106/paripex/4801859.
Angkasekwinai et al., Safety and Efficacy of Ivermectin for the Prevention and Treatment of COVID-19: A Double-Blinded Randomized Placebo-Controlled Study, Antibiotics, doi:10.3390/antibiotics11060796.
Abbas et al., The Effect of Ivermectin on Reducing Viral Symptoms in Patients with Mild COVID-19, Indian Journal of Pharmaceutical Sciences, doi:10.36468/pharmaceutical-sciences.spl.416.
Ahsan et al., Clinical Variants, Characteristics, and Outcomes Among COVID-19 Patients: A Case Series Analysis at a Tertiary Care Hospital in Karachi, Pakistan, Cureus, doi:10.7759/cureus.14761.
Chamie, J., More about Ivermectin. Is this study a fraud?, juanchamie.substack.com/p/more-about-ivermectin-is-this-study.
Borody et al., Combination Therapy For COVID-19 Based on Ivermectin in an Australian Population, TrialSite News, www.trialsitenews.com/a/combination-therapy-for-covid-19-based-on-ivermectin-in-an-australian-population.
Buonfrate et al., High dose ivermectin for the early treatment of COVID-19 (COVER study): a randomised, double-blind, multicentre, phase II, dose-finding, proof of concept trial, International Journal of Antimicrobial Agents, doi:10.1016/j.ijantimicag.2021.106516.
Cadegiani et al., Early COVID-19 Therapy with azithromycin plus nitazoxanide, ivermectin or hydroxychloroquine in Outpatient Settings Significantly Improved COVID-19 outcomes compared to Known outcomes in untreated patients, New Microbes and New Infections, doi:10.1016/j.nmni.2021.100915.
Carvallo et al., Study of the Efficacy and Safety of Topical Ivermectin + Iota-Carrageenan in the Prophylaxis against COVID-19 in Health Personnel, Journal of Biomedical Research and Clinical Investigation, doi:10.31546/2633-8653.1007.
Carvallo (B) et al., Usefulness of Topic Ivermectin and Carrageenan to Prevent Contagion of Covid 19 (IVERCAR), NCT04425850, clinicaltrials.gov/ct2/show/results/NCT04425850.
Carvallo (C) et al., Safety and Efficacy of the Combined Use of Ivermectin, Dexamethasone, Enoxaparin and Aspirina against COVID-19 the I.D.E.A. Protocol, Journal of Clinical Trials, 11:459 (preprint 9/15/20), www.longdom.org/open-access/safety-and-efficacy-of-the-combined-use-of-ivermectin-dexamethasone-enoxaparin-and-aspirina-against-covid19-the-idea-protocol-70290.html.
de Jesús Ascencio-Montiel et al., A Multimodal Strategy to Reduce the Risk of Hospitalization/death in Ambulatory Patients with COVID-19, Archives of Medical Research, doi:10.1016/j.arcmed.2022.01.002.
de la Rocha et al., Ivermectin compared with placebo in the clinical course in Mexican patients with asymptomatic and mild COVID-19: a randomized clinical trial, BMC Infectious Diseases, doi:10.1186/s12879-022-07890-6.
Elavarasi et al., Clinical features, demography, and predictors of outcomes of SARS-CoV-2 infection at a tertiary care hospital in India: A cohort study, Lung India, doi:10.4103/lungindia.lungindia_493_21.
Ferreira et al., Outcomes associated with Hydroxychloroquine and Ivermectin in hospitalized patients with COVID-19: a single-center experience, Revista da Associação Médica Brasileira, doi:10.1590/1806-9282.20210661.
Hashmi et al., Ivermectin for patients admitted to an ICU with COVID-19: REMAP-CAP randomized controlled trial, Critical Care Reviews, CCR24, criticalcarereviews.com/meetings/ccr24#1.
Hazan (B) et al., Effectiveness of ivermectin-based multidrug therapy in severely hypoxic, ambulatory COVID-19 patients, medRxiv, doi:10.1101/2021.07.06.21259924.
Mikamo et al., Efficacy and safety of ivermectin in patients with mild COVID-19 in Japan and Thailand, Journal of Infection and Chemotherapy, doi:10.1016/j.jiac.2023.12.012.
Mustafa et al., Pattern of medication utilization in hospitalized patients with COVID-19 in three District Headquarters Hospitals in the Punjab province of Pakistan, Exploratory Research in Clinical and Social Pharmacy, doi:10.1016/j.rcsop.2021.100101.
Qadeer et al., Ivermectin A Potential Treatment In Covid-19, Related to Critical Illness, Pakistan Journal of Medical and Health Sciences, doi:10.53350/pjmhs2216824.
Ravikirti et al., Association between Ivermectin treatment and mortality in Covid-19: A hospital-based case-control study, Research Square, doi:10.21203/rs.3.rs-1522422/v1.
Rezai et al., Non-effectiveness of Ivermectin on Inpatients and Outpatients With COVID-19; Results of Two Randomized, Double-Blinded, Placebo-Controlled Clinical Trials, Frontiers in Medicine, doi:10.3389/fmed.2022.919708.
Rezai (B) et al., Non-effectiveness of Ivermectin on Inpatients and Outpatients With COVID-19; Results of Two Randomized, Double-Blinded, Placebo-Controlled Clinical Trials, Frontiers in Medicine, doi:10.3389/fmed.2022.919708.
Roy et al., Outcome of Different Therapeutic Interventions in Mild COVID-19 Patients in a Single OPD Clinic of West Bengal: A Retrospective study, medRxiv, doi:10.1101/2021.03.08.21252883.
Samajdar et al., Ivermectin and Hydroxychloroquine for Chemo-Prophylaxis of COVID-19: A Questionnaire Survey of Perception and Prescribing Practice of Physicians vis-a-vis Outcomes, Journal of the Association of Physicians India, 69:11, www.researchgate.net/publication/356294136_Ivermectin_and_Hydroxychloroquine_for_Chemo-Prophylaxis_of_COVID-19_A_Questionnaire_Survey_of_Perception_and_Prescribing_Practice_of_Physicians_vis-a-vis_Outcomes.
Schilling et al., Pharmacometrics of high dose ivermectin in early COVID-19: an open label, randomized, controlled adaptive platform trial (PLATCOV), eLife, doi:10.7554/eLife.83201.
Siripongboonsitti et al., A Randomized Trial to Assess the Acceleration of Viral Clearance by the Combination Favipiravir/Ivermectin/Niclosamide in Mild-to-Moderate COVID-19 Adult Patients (FINCOV), Journal of Infection and Public Health, doi:10.1016/j.jiph.2024.03.030.
Soto et al., Mortality and associated risk factors in patients hospitalized due to COVID-19 in a Peruvian reference hospital, PLOS ONE, doi:10.1371/journal.pone.0264789.
Szente Fonseca et al., Risk of Hospitalization for Covid-19 Outpatients Treated with Various Drug Regimens in Brazil: Comparative Analysis, Travel Medicine and Infectious Disease, doi:10.1016/j.tmaid.2020.101906.
Thairu et al., A Comparison of Ivermectin and Non Ivermectin Based Regimen for COVID-19 in Abuja: Effects on Virus Clearance, Days-to-discharge and Mortality, Journal of Pharmaceutical Research International, doi:10.9734/jpri/2022/v34i44A36328.
Zubair et al., The effect of ivermectin on non-severe and severe COVID-19 disease and gender-based difference of its effectiveness, Monaldi Archives for Chest Disease, doi:10.4081/monaldi.2022.2062.
Treanor et al., Efficacy and Safety of the Oral Neuraminidase Inhibitor Oseltamivir in Treating Acute Influenza: A Randomized Controlled Trial, JAMA, 2000, 283:8, 1016-1024, doi:10.1001/jama.283.8.1016.
McLean et al., Impact of Late Oseltamivir Treatment on Influenza Symptoms in the Outpatient Setting: Results of a Randomized Trial, Open Forum Infect. Dis. September 2015, 2:3, doi:10.1093/ofid/ofv100.
Ikematsu et al., Baloxavir Marboxil for Prophylaxis against Influenza in Household Contacts, New England Journal of Medicine, doi:10.1056/NEJMoa1915341.
Hayden et al., Baloxavir Marboxil for Uncomplicated Influenza in Adults and Adolescents, New England Journal of Medicine, doi:10.1056/NEJMoa1716197.
Kumar et al., Combining baloxavir marboxil with standard-of-care neuraminidase inhibitor in patients hospitalised with severe influenza (FLAGSTONE): a randomised, parallel-group, double-blind, placebo-controlled, superiority trial, The Lancet Infectious Diseases, doi:10.1016/S1473-3099(21)00469-2.
Korves et al., SARS-CoV-2 Genetic Variants and Patient Factors Associated with Hospitalization Risk, medRxiv, doi:10.1101/2024.03.08.24303818.
Faria et al., Genomics and epidemiology of the P.1 SARS-CoV-2 lineage in Manaus, Brazil, Science, doi:10.1126/science.abh2644.
Nonaka et al., SARS-CoV-2 variant of concern P.1 (Gamma) infection in young and middle-aged patients admitted to the intensive care units of a single hospital in Salvador, Northeast Brazil, February 2021, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.08.003.
Karita et al., Trajectory of viral load in a prospective population-based cohort with incident SARS-CoV-2 G614 infection, medRxiv, doi:10.1101/2021.08.27.21262754.
Zavascki et al., Advanced ventilatory support and mortality in hospitalized patients with COVID-19 caused by Gamma (P.1) variant of concern compared to other lineages: cohort study at a reference center in Brazil, Research Square, doi:10.21203/rs.3.rs-910467/v1.
Willett et al., The hyper-transmissible SARS-CoV-2 Omicron variant exhibits significant antigenic change, vaccine escape and a switch in cell entry mechanism, medRxiv, doi:10.1101/2022.01.03.21268111.
Peacock et al., The SARS-CoV-2 variant, Omicron, shows rapid replication in human primary nasal epithelial cultures and efficiently uses the endosomal route of entry, bioRxiv, doi:10.1101/2021.12.31.474653.
Babalola et al., Ivermectin shows clinical benefits in mild to moderate COVID19: A randomised controlled double-blind, dose-response study in Lagos, QJM: An International Journal of Medicine, doi:10.1093/qjmed/hcab035.
Xu et al., A study of impurities in the repurposed COVID-19 drug hydroxychloroquine sulfate by UHPLC-Q/TOF-MS and LC-SPE-NMR, Rapid Communications in Mass Spectrometry, doi:10.1002/rcm.9358.
Ostrov et al., Highly Specific Sigma Receptor Ligands Exhibit Anti-Viral Properties in SARS-CoV-2 Infected Cells, Pathogens, doi:10.3390/pathogens10111514.
Alsaidi et al., Griffithsin and Carrageenan Combination Results in Antiviral Synergy against SARS-CoV-1 and 2 in a Pseudoviral Model, Marine Drugs, doi:10.3390/md19080418.
Andreani et al., In vitro testing of combined hydroxychloroquine and azithromycin on SARS-CoV-2 shows synergistic effect, Microbial Pathogenesis, doi:10.1016/j.micpath.2020.104228.
Wan et al., Synergistic inhibition effects of andrographolide and baicalin on coronavirus mechanisms by downregulation of ACE2 protein level, Scientific Reports, doi:10.1038/s41598-024-54722-5.
Said et al., The effect of Nigella sativa and vitamin D3 supplementation on the clinical outcome in COVID-19 patients: A randomized controlled clinical trial, Frontiers in Pharmacology, doi:10.3389/fphar.2022.1011522.
Fiaschi et al., In Vitro Combinatorial Activity of Direct Acting Antivirals and Monoclonal Antibodies against the Ancestral B.1 and BQ.1.1 SARS-CoV-2 Viral Variants, Viruses, doi:10.3390/v16020168.
Xing et al., Published anti-SARS-CoV-2 in vitro hits share common mechanisms of action that synergize with antivirals, Briefings in Bioinformatics, doi:10.1093/bib/bbab249.
Chen et al., Synergistic Inhibition of SARS-CoV-2 Replication Using Disulfiram/Ebselen and Remdesivir, ACS Pharmacology & Translational Science, doi:10.1021/acsptsci.1c00022.
Hempel et al., Synergistic inhibition of SARS-CoV-2 cell entry by otamixaban and covalent protease inhibitors: pre-clinical assessment of pharmacological and molecular properties, Chemical Science, doi:10.1039/D1SC01494C.
Schultz et al., Pyrimidine inhibitors synergize with nucleoside analogues to block SARS-CoV-2, Nature, doi:10.1038/s41586-022-04482-x.
Ohashi et al., Potential anti-COVID-19 agents, cepharanthine and nelfinavir, and their usage for combination treatment, iScience, doi:10.1016/j.isci.2021.102367.
Al Krad et al., The protease inhibitor Nirmatrelvir synergizes with inhibitors of GRP78 to suppress SARS-CoV-2 replication, bioRxiv, doi:10.1101/2025.03.09.642200.
Singh et al., The relationship between viral clearance rates and disease progression in early symptomatic COVID-19: a systematic review and meta-regression analysis, Journal of Antimicrobial Chemotherapy, doi:10.1093/jac/dkae045.
WHO, Therapeutics and COVID-19: Living Guideline 31 March 2021, apps.who.int/iris/bitstream/handle/10665/340374/WHO-2019-nCoV-therapeutics-2021.1-eng.pdf.
Kory (B), P., FLCCC Alliance Statement on the Irregular Actions of Public Health Agencies and the Widespread Disinformation Campaign Against Ivermectin, covid19criticalcare.com/wp-content/uploads/2021/05/CLEAN-FLCCC-STATEMENT-AGAINST-THE-GLOBAL-IVERMECTIN-DISINFORMATION-CAMPAIGN-5.11.2021.pdf.
COVID-NMA, COVID-NMA weekly update, May 14, 2021, web.archive.org/web/20210514184958/https://www.covid-nma.com/news/.
Reuters, WHO joins Europe, Merck in recommending against ivermectin for COVID-19, news.trust.org/item/20210331135538-tajza/.
Rochwerg et al., Remdesivir for severe covid-19: a clinical practice guideline, BMJ, doi:10.1136/bmj.m2924.
Yagisawa et al., Global trends in clinical studies of ivermectin in COVID-19, The Japanese Journal of Antibiotics, 74-1, Mar 2021, jja-contents.wdc-jp.com/pdf/JJA74/74-1-open/74-1_44-95.pdf.
Merck, Merck Statement on Ivermectin use During the COVID-19 Pandemic, www.merck.com/news/merck-statement-on-ivermectin-use-during-the-covid-19-pandemic/.
Zatloukal et al., News report on In Vitro results from the research institute of Prof. Zatloukal, www.servustv.com/videos/aa-27juub3a91w11/.
Zaidi et al., The mechanisms of action of ivermectin against SARS-CoV-2—an extensive review, The Journal of Antibiotics, doi:10.1038/s41429-021-00491-6.
Wehbe et al., Repurposing Ivermectin for COVID-19: Molecular Aspects and Therapeutic Possibilities, Front. Immunol., doi:10.3389/fimmu.2021.663586.
Kalfas et al., The therapeutic potential of ivermectin for COVID-19: a systematic review of mechanisms and evidence, medRxiv, doi:10.1101/2020.11.30.20236570.
Jans et al., Ivermectin as a Broad-Spectrum Host-Directed Antiviral: The Real Deal?, Cells 2020, 9:9, 2100, doi:10.3390/cells9092100.
Heidary et al., Ivermectin: a systematic review from antiviral effects to COVID-19 complementary regimen, The Journal of Antibiotics, 73, 593–602, doi:10.1038/s41429-020-0336-z.
Chowdhury et al., A Comparative Study on Ivermectin-Doxycycline and Hydroxychloroquine-Azithromycin Therapy on COVID-19 Patients, Eurasian Journal of Medicine and Oncology, doi:10.14744/ejmo.2021.16263.
Espitia-Hernandez et al., Effects of Ivermectin-azithromycin-cholecalciferol combined therapy on COVID-19 infected patients: A proof of concept study, Biomedical Research, 31:5, www.biomedres.info/biomedical-research/effects-of-ivermectinazithromycincholecalciferol-combined-therapy-on-covid19-infected-patients-a-proof-of-concept-study-14435.html.
Mahmud et al., Ivermectin in combination with doxycycline for treating COVID-19 symptoms: a randomized trial, Journal of International Medical Research, doi:10.5061/dryad.qjq2bvqf6.
Chaccour (B) et al., The effect of early treatment with ivermectin on viral load, symptoms and humoral response in patients with non-severe COVID-19: A pilot, double-blind, placebo-controlled, randomized clinical trial, eClinicalMedicine, doi:10.1016/j.eclinm.2020.100720.
Ghauri et al., Ivermectin Use Associated with Reduced Duration of Covid-19 Febrile Illness in a Community Setting, International Journal of Clinical Studies & Medical Case Reports, doi:10.46998/IJCMCR.2021.13.000320.
Ravikirti (B) et al., Ivermectin as a potential treatment for mild to moderate COVID-19: A double blind randomized placebo-controlled trial, Journal of Pharmacy & Pharmaceutical Sciences, doi:10.18433/jpps32105.
Bukhari et al., Efficacy of Ivermectin in COVID-19 Patients with Mild to Moderate Disease, medRxiv, doi:10.1101/2021.02.02.21250840.
Mohan et al., Single-dose oral ivermectin in mild and moderate COVID-19 (RIVET-COV): a single-centre randomized, placebo-controlled trial, Journal of Infection and Chemotherapy, doi:10.1016/j.jiac.2021.08.021.
Elalfy et al., Effect of a combination of Nitazoxanide, Ribavirin and Ivermectin plus zinc supplement (MANS.NRIZ study) on the clearance of mild COVID-1, Journal of Medical Virology, doi:10.1002/jmv.26880.
Chahla et al., Randomized trials - Ivermectin repurposing for COVID-19 treatment of outpatients with mild disease in primary health care centers, Research, Society and Development, doi:10.33448/rsd-v11i8.30844.
Mourya et al., Comparative Analytical Study of Two Different Drug Regimens in Treatment of Covid 19 Positive Patients in Index Medical College Hospital and Research Center, Indore, India, International Journal of Health and Clinical Research, 4:6, ijhcr.com/index.php/ijhcr/article/view/1263.
Loue et al., Ivermectin and COVID-19 in Care Home: Case Report, J. Infectious Diseases and Epidemiology, doi:10.23937/2474-3658/1510202.
Merino et al., Ivermectin and the odds of hospitalization due to COVID-19: evidence from a quasi-experimental analysis based on a public intervention in Mexico City, Preprint, web.archive.org/web/20211218011849/https://files.osf.io/v1/resources/r93g4/providers/osfstorage/609085945533b4031ee1c789?action=download&direct&version=1.
Faisal et al., Potential use of azithromycin alone and in combination with ivermectin in fighting against the symptoms of COVID-19, The Professional Medical Journal, doi:10.29309/TPMJ/2021.28.05.5867.
Aref et al., Clinical, Biochemical and Molecular Evaluations of Ivermectin Mucoadhesive Nanosuspension Nasal Spray in Reducing Upper Respiratory Symptoms of Mild COVID-19, International Journal of Nanomedicine, doi:10.2147/IJN.S313093.
Mayer et al., Safety and Efficacy of a MEURI Program for the Use of High Dose Ivermectin in COVID-19 Patients, Frontiers in Public Health, doi:10.3389/fpubh.2022.813378.
Manomaipiboon et al., Efficacy and safety of ivermectin in the treatment of mild-to-moderate COVID-19 infection: A randomized, double blind, placebo, controlled trial, Trials, doi:10.1186/s13063-022-06649-3.
Khan et al., Ivermectin treatment may improve the prognosis of patients with COVID-19, Archivos de Bronconeumología, doi:10.1016/j.arbres.2020.08.007.
Hashim et al., Controlled randomized clinical trial on using Ivermectin with doxycycline for treating COVID-19 patients in Baghdad, Iraq, Iraqi Journal of Medical Science, 19:1, www.iraqijms.net/upload/pdf/iraqijms60db8b76d3b1e.pdf.
Budhiraja et al., Clinical Profile of First 1000 COVID-19 Cases Admitted at Tertiary Care Hospitals and the Correlates of their Mortality: An Indian Experience, medRxiv, doi:10.1101/2020.11.16.20232223.
Okumuş et al., Evaluation of the Effectiveness and Safety of Adding Ivermectin to Treatment in Severe COVID-19 Patients, BMC Infectious Diseases, doi:10.1186/s12879-021-06104-9.
Lima-Morales et al., Effectiveness of a multidrug therapy consisting of ivermectin, azithromycin, montelukast and acetylsalicylic acid to prevent hospitalization and death among ambulatory COVID-19 cases in Tlaxcala, Mexico, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.02.014.
Huvemek, Kovid-19 - Huvemek® Phase 2 clinical trial, Press Release, huvemec.bg/covid-19-huvemec-klinichno-izpitanie/za-isledvaneto/.
Baguma et al., Characteristics of the COVID-19 patients treated at Gulu Regional Referral Hospital, Northern Uganda: A cross-sectional study, Research Square, doi:10.21203/rs.3.rs-1193578/v1.
Shimizu et al., Ivermectin administration is associated with lower gastrointestinal complications and greater ventilator-free days in ventilated patients with COVID-19: A propensity score analysis, Journal of Infection and Chemotherapy, doi:10.1016/j.jiac.2021.12.024.
Aref (B) et al., Possible Role of Ivermectin Mucoadhesive Nanosuspension Nasal Spray in Recovery of Post-COVID-19 Anosmia, Infection and Drug Resistance, doi:10.2147/IDR.S381715.
Varnaseri et al., Ivermectin as a Potential Addition to the Limited Anti-COVID-19 Arsenal: A Double-Blinded Clinical Trial, Jundishapur Journal of Health Sciences, doi:10.5812/jjhs-146703.
Behera et al., Role of ivermectin in the prevention of SARS-CoV-2 infection among healthcare workers in India: A matched case-control study, PLOS ONE, doi:10.1371/journal.pone.0247163.
Bernigaud et al., Ivermectin benefit: from scabies to COVID-19, an example of serendipity, Annals of Dermatology and Venereology, doi:10.1016/j.annder.2020.09.231.
Alam et al., Ivermectin as Pre-exposure Prophylaxis for COVID-19 among Healthcare Providers in a Selected Tertiary Hospital in Dhaka – An Observational Study, European Journal of Medical and Health Sciences, doi:10.24018/ejmed.2020.2.6.599.
Chahla (B) et al., Intensive Treatment With Ivermectin and Iota-Carrageenan as Pre-exposure Prophylaxis for COVID-19 in Health Care Workers From Tucuman, Argentina, American Journal of Therapeutics, doi:10.1097/MJT.0000000000001433.
Behera (B) et al., Prophylactic Role of Ivermectin in Severe Acute Respiratory Syndrome Coronavirus 2 Infection Among Healthcare Workers, Cureus, doi:10.7759/cureus.16897.
Seet et al., Positive impact of oral hydroxychloroquine and povidone-iodine throat spray for COVID-19 prophylaxis: an open-label randomized trial, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.04.035.
Morgenstern et al., Ivermectin as a SARS-CoV-2 Pre-Exposure Prophylaxis Method in Healthcare Workers: A Propensity Score-Matched Retrospective Cohort Study, Cureus, doi:10.7759/cureus.17455.
Mondal et al., Prevalence of COVID-19 Infection and Identification of Risk Factors among Asymptomatic Healthcare Workers: A Serosurvey Involving Multiple Hospitals in West Bengal, Journal of the Indian Medical Association, 119:5, onlinejima.com/read_journals.php?article=683.
Kerr et al., Ivermectin Prophylaxis Used for COVID-19: A Citywide, Prospective, Observational Study of 223,128 Subjects Using Propensity Score Matching, Cureus, doi:10.7759/cureus.21272.
Ahmed et al., A five day course of ivermectin for the treatment of COVID-19 may reduce the duration of illness, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2020.11.191.
Biber et al., The effect of ivermectin on the viral load and culture viability in early treatment of non-hospitalized patients with mild COVID-19 – A double-blind, randomized placebo-controlled trial, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2022.07.003.
Krolewiecki et al., Antiviral effect of high-dose ivermectin in adults with COVID-19: A proof-of-concept randomized trial, eClinicalMedicine, doi:10.1016/j.eclinm.2021.100959.
Gorial et al., Effectiveness of Ivermectin as add-on Therapy in COVID-19 Management (Pilot Trial), medRxiv, doi:10.1101/2020.07.07.20145979.
Camprubí et al., Lack of efficacy of standard doses of ivermectin in severe COVID-19 patients, PLoS ONE, 15:11, doi:10.1371/journal.pone.0242184.
Spoorthi et al., Utility of Ivermectin and Doxycycline combination for the treatment of SARSCoV-2, IAIM, 2020, 7:10, 177-182, iaimjournal.com/wp-content/uploads/2020/10/iaim_2020_0710_23.pdf.
Pott-Junior et al., Use of ivermectin in the treatment of Covid-19: a pilot trial, Toxicology Reports, doi:10.1016/j.toxrep.2021.03.003.
Abd-Elsalam et al., Clinical Study Evaluating the Efficacy of Ivermectin in COVID-19 Treatment: A Randomized Controlled Study, Journal of Medical Virology, doi:10.1002/jmv.27122.
George et al., Single Dose of Ivermectin is not Useful in Patients with Hematological Disorders and COVID-19 Illness: A Phase II B Open Labelled Randomized Controlled Trial, Indian Journal of Hematology and Blood Transfusion, doi:10.1007/s12288-022-01546-w.
Shouman (B) et al., Use of Ivermectin as a Potential Chemoprophylaxis for COVID-19 in Egypt: A Randomised Clinical Trial, Journal of Clinical and Diagnostic Research, doi:10.7860/JCDR/2021/46795.14529.
Bhattacharya et al., Observational Study on Clinical Features, Treatment and Outcome of COVID 19 in a tertiary care Centre in India- a retrospective case series, Int. J. Scientific Research, doi:10.36106/ijsr/7232245.
Adams, B., Merck must do a new trial for faltering $425M COVID-19 drug the U.S. government asked it to buy, Fierce Biotech, www.fiercebiotech.com/biotech/merck-s-must-do-a-new-trial-for-faltering-425m-covid-drug-u-s-government-asked-it-to-buy.
Jayk Bernal et al., Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients, New England Journal of Medicine, doi:10.1056/NEJMoa2116044.
Khan (B), T., Merck Signs ~$1.2B Supply Agreement with US Government for Molnupiravir to Treat COVID-19, PharmaShots, pharmashots.com/61076/merck-signs-1-2b-supply-agreement-with-us-government-for-molnupiravir-to-treat-covid-19/.
Genetic Engineering and Biotechnology News, Merck to Seek FDA EUA for COVID-19 Pill after Positive Phase III Data, www.genengnews.com/news/merck-to-seek-fda-eua-for-covid-19-pill-after-positive-phase-iii-data/.
Scheim (D), D., Merck’s deadly Vioxx playbook, redux: a debunked smear campaign against its competing drug—the FDA-approved, Nobel prize-honored ivermectin, TrialsSite News, trialsitenews.com/mercks-deadly-vioxx-playbook-redux-a-debunked-smear-campaign-against-its-competing-drug-the-fda-approved-nobel-prize-honored-ivermectin/.
Pfeiffer, M., Analysis of the FDA's recommendation on ivermectin, twitter.com/marybethpf/status/1370182744718856193.
Charilaou et al., Acetaminophen Toxicity: Trends in Hospitalization and Their Outcomes in United States from 2002-2011, American Journal of Gastroenterology, doi:10.14309/00000434-201610001-01012.
Wijewickrema et al., Efficacy and safety of oral ivermectin in the treatment of mild to moderate Covid-19 patients: a multi-centre double-blind randomized controlled clinical trial, BMC Infectious Diseases, doi:10.1186/s12879-024-09563-y.
Rezk et al., miRNA-223-3p, miRNA- 2909 and Cytokines Expression in COVID-19 Patients Treated with Ivermectin, Zagazig University Medical Journal, doi:10.21608/zumj.2021.92746.2329.
Podder et al., Outcome of ivermectin treated mild to moderate COVID-19 cases: a single-centre, open-label, randomised controlled study, IMC J. Med. Science, doi:10.3329/imcjms.v14i2.52826.
Chachar et al., Effectiveness of Ivermectin in SARS-CoV-2/COVID-19 Patients, International Journal of Sciences, 9:31-35, doi:10.18483/ijSci.2378.
Rajter et al., Use of Ivermectin is Associated with Lower Mortality in Hospitalized Patients with COVID-19 (ICON study), Chest, doi:10.1016/j.chest.2020.10.009.
NIH, COVID-19 Treatment Guidelines: Ivermectin, www.covid19treatmentguidelines.nih.gov/therapies/antiviral-therapy/ivermectin/.
Yim (B), P., Grotesque conflicts of interest on NIH ivermectin non-recommendation, TrialSite News, trialsitenews.com/grotesque-conflicts-of-interest-on-nih-ivermectin-non-recommendation/.
trialsitenews.com, trialsitenews.com/nih-covid-19-panel-member-received-massive-windfall-from-ivermectin-recommendation/.
covid19treatmentguidelines.nih.gov, www.covid19treatmentguidelines.nih.gov/about-the-guidelines/panel-financial-disclosure/.
trialsitenews.com (B), trialsitenews.com/grotesque-conflicts-of-interest-on-nih-ivermectin-non-recommendation/.
files.covid19treatmentguidelines.nih.gov, files.covid19treatmentguidelines.nih.gov/guidelines/archive/covid19treatmentguidelines-08-27-2020.pdf.
actgnetwork.org, actgnetwork.org/2021/07/29/actg-launches-study-evaluating-the-effects-of-an-arv-change-among-people-living-with-hiv-who-experience-excessive-weight-gain/.
Bitterman et al., Comparison of Trials Using Ivermectin for COVID-19 Between Regions With High and Low Prevalence of Strongyloidiasis, JAMA Network Open, doi:10.1001/jamanetworkopen.2022.3079.
Wagstaff (C) et al., In vitro investigations of ivermectin as an antiviral agent, Ivermectin Global Sumit, vimeo.com/554860553#t=1h32m0s.
Lespine et al., Influence of the route of administration on efficacy and tissue distribution of ivermectin in goat, Veterinary Parasitology, doi:10.1016/j.vetpar.2004.11.028.
Lifschitz et al., Comparative distribution of ivermectin and doramectin to parasite location tissues in cattle, Veterinary Parasitology, doi:10.1016/s0304-4017(99)00175-2.
Bray et al., Ivermectin and COVID-19: A report in Antiviral Research, widespread interest, an FDA warning, two letters to the editor and the authors' responses, Antiviral Res., doi:10.1016/j.antiviral.2020.104805.
Jerusalem Post, Israeli scientist says COVID-19 could be treated for under $1/day, www.jpost.com/health-science/israeli-scientist-says-covid-19-could-be-treated-for-under-1day-675612.
Fox, C., Did Dismissals of Safe Outpatient Drugs Cause Needless Covid Deaths? Dissenting Doctors Say Yes, RealClearInvestigations, www.realclearinvestigations.com/articles/2021/12/21/did_dismissals_of_safe_outpatient_drugs_cause_needless_covid_deaths_dissenting_doctors_say_yes_808045.html.
Efimenko et al., Treatment with Ivermectin Is Associated with Decreased Mortality in COVID-19 Patients: Analysis of a National Federated Database, International Journal of Infectious Diseases, doi:10.1016/j.ijid.2021.12.096.
Kory (D), P., The Criminal Censorship of Ivermectin's Efficacy By The High-Impact Medical Journals - Part 1, Pierre Kory’s Medical Musings, pierrekory.substack.com/p/the-criminal-censorship-of-ivermectins.
Kory (E), P., The Criminal Censorship Of Ivermectin By The High Impact Medical Journals - Part 2, Pierre Kory’s Medical Musings, pierrekory.substack.com/p/the-criminal-censorship-of-ivermectin.
Kory (F), P., The Criminal Censorship Of Ivermectin By The High Impact Medical Journals - Part 3, Pierre Kory’s Medical Musings, pierrekory.substack.com/p/the-criminal-censorship-of-ivermectin-418.
medicospelavidacovid19.com.br, medicospelavidacovid19.com.br/editoriais/folha-de-s-paulo-revela-numeros-de-david-uip-veja-a-comparacao-com-medicos-que-fazem-tratamento-precoce/.
Rothstein, H., Publication Bias in Meta-Analysis: Prevention, Assessment and Adjustments, www.wiley.com/en-ae/Publication+Bias+in+Meta+Analysis:+Prevention,+Assessment+and+Adjustments-p-9780470870143.
Stanley et al., Meta-regression approximations to reduce publication selection bias, Research Synthesis Methods, doi:10.1002/jrsm.1095.
Rücker et al., Arcsine test for publication bias in meta-analyses with binary outcomes, Statistics in Medicine, doi:10.1002/sim.2971.
Peters, J., Comparison of Two Methods to Detect Publication Bias in Meta-analysis, JAMA, doi:10.1001/jama.295.6.676.
Moreno et al., Assessment of regression-based methods to adjust for publication bias through a comprehensive simulation study, BMC Medical Research Methodology, doi:10.1186/1471-2288-9-2.
Macaskill et al., A comparison of methods to detect publication bias in meta-analysis, Statistics in Medicine, doi:10.1002/sim.698.
Egger et al., Bias in meta-analysis detected by a simple, graphical test, BMJ, doi:10.1136/bmj.315.7109.629.
Harbord et al., A modified test for small-study effects in meta-analyses of controlled trials with binary endpoints, Statistics in Medicine, doi:10.1002/sim.2380.
Evans, R., Tough on Crime? Pfizer and the CIHR, Healthcare Policy, 5:4, www.ncbi.nlm.nih.gov/pmc/articles/PMC2875889/.
Areskog et al., Dexamethasone treatment interferes with the pharmacokinetics of ivermectin in young cattle, Veterinary Parasitology, doi:10.1016/j.vetpar.2012.07.011.
Goodkin, M., Are Major Ivermectin Studies Designed for Failure?, trialsitenews.com/are-major-ivermectin-studies-designed-for-failure/.
Zhang (B) et al., Rho-GTPases subfamily: cellular defectors orchestrating viral infection, Cellular & Molecular Biology Letters, doi:10.1186/s11658-025-00722-w.
Saha (D) et al., Inhaled Dry Powder of Antiviral Agents: A Promising Approach to Treating Respiratory Viral Pathogens, Viruses, doi:10.3390/v17020252.
Ulloa-Aguilar et al., The Nucleolus and Its Interactions with Viral Proteins Required for Successful Infection, Cells, doi:10.3390/cells13181591.
Enyeji et al., Effective Treatment of COVID-19 Infection with Repurposed Drugs: Case Reports, Viral Immunology, doi:10.1089/vim.2024.0034.
Wimalawansa, S., Unlocking Insights: Navigating COVID-19 Challenges and Emulating Future Pandemic Resilience Strategies with Strengthening Natural Immunity, Heliyon, doi:10.1016/j.heliyon.2024.e34691.
Mehraeen et al., Treatments for Olfactory Dysfunction in COVID-19: A Systematic Review, International Archives of Otorhinolaryngology, doi:10.1055/s-0044-1786046.
Scheim (E) et al., Back to the Basics of SARS-CoV-2 Biochemistry: Microvascular Occlusive Glycan Bindings Govern Its Morbidities and Inform Therapeutic Responses, Viruses, doi:10.3390/v16040647.
Yagisawa (B) et al., Global trends in clinical trials of ivermectin for COVID-19—Part 2, The Japanese Journal of Antibiotics, doi:10.11553/antibiotics.77.1_45.
Yemeke et al., Impact of the COVID-19 pandemic on the quality of medical products in Zimbabwe: a qualitative study based on key informant interviews with health system stakeholders, BMJ Open, doi:10.1136/bmjopen-2022-068923.
Kory (G), P., The Global War on Ivermectin, International Covid Summit III, European Parliament, Brussels, covid19criticalcare.com/wp-content/uploads/2023/05/GLOBAL-WAR-ON-IVERMECTIN-PARLIAMENT.pdf.
Babalola (B) et al., The Place of Ivermectin in the Management of Covid-19: State of the Evidence, Medical Research Archives, doi:10.18103/mra.v11i4.3778.
Loo et al., Recent Advances in Inhaled Nanoformulations of Vaccines and Therapeutics Targeting Respiratory Viral Infections, Pharmaceutical Research, doi:10.1007/s11095-023-03520-1.
Al-kuraishy et al., Central effects of Ivermectin in alleviation of Covid-19-induced dysautonomia, Current Drug Targets, doi:10.2174/1389450123666220810102406.
Schwartz, E., Does ivermectin have a place in the treatment of mild Covid-19?, New Microbes and New Infections, doi:10.1016/j.nmni.2022.100989.
Marques et al., Ivermectin as a possible treatment for COVID-19: a review of the 2022 protocols, Brazilian Journal of Biology, doi:10.1590/1519-6984.258325.
Semiz, S., SIT1 transporter as a potential novel target in treatment of COVID-19, Biomolecular Concepts, doi:10.1515/bmc-2021-0017.
Low et al., Repositioning Ivermectin for Covid-19 treatment: Molecular mechanisms of action against SARS-CoV-2 replication, Biochimica et Biophysica Acta (BBA) - Molecular Basis of Disease, doi:10.1016/j.bbadis.2021.166294.
Fordham et al., The uses and abuses of systematic reviews, OSF Preprints, doi:10.31219/osf.io/mp4f2.
Kow et al., Pitfalls in Reporting Sample Size Calculation Across Randomized Controlled Trials Involving Ivermectin for the treatment of COVID-19, American Journal of Therapeutics, doi:10.1097/MJT.0000000000001441.
Santin et al., Ivermectin: a multifaceted drug of Nobel prize-honored distinction with indicated efficacy against a new global scourge, COVID-19, New Microbes and New Infections, doi:10.1016/j.nmni.2021.100924.
Adegboro et al., A review of the anti-viral effects of ivermectin, African Journal of Clinical and Experimental Microbiology, doi:10.4314/ajcem.v22i3.2.
Turkia, M., A Continuation of a Timeline of Ivermectin-Related Events in the COVID-19 Pandemic [June 30, 2021], ResearchGate, doi:10.13140/RG.2.2.16973.36326.
Jagiasi et al., Variation in therapeutic strategies for the management of severe COVID-19 in India- A nationwide cross-sectional survey, The International Journal of Clinical Practice, doi:10.1111/ijcp.14574.
Lind et al., Increase in Outpatient Ivermectin Dispensing in the US During the COVID-19 Pandemic: A Cross-Sectional Analysis, Journal of General Internal Medicine, doi:10.1007/s11606-021-06948-6.
Wang (B) et al., Minimum manufacturing costs, national prices and estimated global availability of new repurposed therapies for COVID-19, medRxiv, doi:10.1101/2021.06.01.21258147.
Turkia (B), M., A timeline of ivermectin-related events in the COVID-19 pandemic, Research Gate, www.researchgate.net/publication/350610718_A_Timeline_of_Ivermectin-Related_Events_in_the_COVID-19_Pandemic_April_3_2021.
Jans (B) et al., The broad spectrum host-directed agent ivermectin as an antiviral for SARS-CoV-2 ?, Biochemical and Biophysical Research Communications, doi:10.1016/j.bbrc.2020.10.042.
Kory (H) et al., Review of the Emerging Evidence Demonstrating the Efficacy of Ivermectin in the Prophylaxis and Treatment of COVID-19, Frontiers in Pharmacology, doi:10.3389/fphar.2021.643369.
Formiga et al., Ivermectin: an award-winning drug with expected antiviral activity against COVID-19, J. Control Release, doi:10.1016/j.jconrel.2020.10.009.
Turkia (C), M., FLCCC Alliance MATH+ ascorbic acid and I-MASK+ ivermectin protocols for COVID-19 — a brief review, ResearchGate, www.researchgate.net/profile/Mika_Turkia/publication/345694745_FLCCC_Alliance_MATH_ascorbic_acid_and_I-MASK_ivermectin_protocols_for_COVID-19_-_A_Brief_Review/links/5fab010f4585150781078260/FLCCC-Alliance-MATH-ascorbic-acid-and-I-MASK-ivermectin-protocols-for-COVID-19-A-Brief-Review.pdf.
Vora et al., White paper on Ivermectin as a potential therapy for COVID-19, Indian Journal of Tuberculosis, doi:10.1016/j.ijtb.2020.07.031.
Ragó et al., Results of a systematic review and meta-analysis of early studies on ivermectin in SARS-CoV-2 infection, GeroScience, doi:10.1007/s11357-023-00756-y.
Kory (I), P., Dr. Pierre Kory Talks About Human Rights and The Big Science Disinformation, www.youtube.com/watch?v=3UTuT9TSRFQ&t=2890s.
Vanhee et al., Substandard and falsified ivermectin tablets obtained for self‐medication during the COVID‐19 pandemic as a source of potential harm, Drug Testing and Analysis, doi:10.1002/dta.3618.
Therapeutic Goods Administration, TGA warns about imports of ivermectin, News Release, December 2021, www.tga.gov.au/news/media-releases/tga-warns-about-imports-ivermectin.
Therapeutic Goods Administration (B), TGA cautions consumers over counterfeit ivermectin, News Release, March 2022, www.tga.gov.au/news/media-releases/tga-cautions-consumers-over-counterfeit-ivermectin.
Huerta León et al., Content and characteristics of ivermectin in master formulations, Revista Cubana de Medicina Militar, 53:4, revmedmilitar.sld.cu/index.php/mil/article/view/45001.
Sheldrick, K., Schedule A: Statement, This Scattrd Corn, web.archive.org/web/20230602194132/https://kylesheldrick.blogspot.com/2023/05/update.html.
Fenton, M., The curious perfect p-value: a case study in defamation and ignorance, www.normanfenton.com/post/the-curious-perfect-p-value-a-case-study-in-defamation-and-ignorance.
Amrhein et al., Scientists rise up against statistical significance, Nature, 567:305-307, www.nature.com/articles/d41586-019-00857-9.
Yeh et al., Parachute use to prevent death and major trauma when jumping from aircraft: randomized controlled trial, BMJ, doi:10.1136/bmj.k5094.
Murai et al., Effect of a Single High Dose of Vitamin D3 on Hospital Length of Stay in Patients With Moderate to Severe COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2020.26848.
BiRD Group, The BBC’s recent article “False Science” disintegrates under scrutiny, bird-group.org/the-bbcs-recent-article-false-science-is-disintegrating-under-scrutiny/.
Elijah, S., How Ivermectin became a Target for the ‘Fraud Detectives.’, TrialSite News, trialsitenews.com/how-ivermectin-became-a-target-for-the-fraud-detectives/.
Chamie-Quintero et al., Ivermectin for COVID-19 in Peru: 14-fold reduction in nationwide excess deaths, p=.002 for effect by state, then 13-fold increase after ivermectin use restricted, OSF Preprints, osf.io/9egh4.
Ontai et al., Early multidrug treatment of SARS-CoV-2 (COVID-19) and decreased case fatality rates in Honduras
, Epidemiology International Journal, doi:10.23880/eij-16000217.
Chamie-Quintero (B), J., The Latest Results of Ivermectin’s Success in Treating Outbreaks of COVID-19, covid19criticalcare.com/ivermectin-in-covid-19/epidemiologic-analyses-on-covid19-and-ivermectin/.
Canga et al., The Pharmacokinetics and Interactions of Ivermectin in Humans—A Mini-review, AAPS J., doi:10.1208/s12248-007-9000-9.
Muñoz et al., Safety and pharmacokinetic profile of fixed-dose ivermectin with an innovative 18mg tablet in healthy adult volunteers, PLoS Negl. Trop. Dis., doi:10.1371/journal.pntd.0006020.
Chaccour (C) et al., Ivermectin to reduce malaria transmission I. Pharmacokinetic and pharmacodynamic considerations regarding efficacy and safety, Malar. J., doi:10.1186/s12936-017-1801-4.
Chiu et al., Absorption, tissue distribution, and excretion of tritium-labeled ivermectin in cattle, sheep, and rat, J. Agric. Food Chem., doi:10.1021/jf00101a015.
O'Reilly, D., A Lifeline from Buenos Aires, rescue.substack.com/p/a-lifeline-from-buenos-aires?r=rcgyu&utm_campaign=post&utm_medium=web&utm_source=copy.
Figueroa et al., Efficacy of a nasal spray containing Iota-Carrageenan in the prophylaxis of COVID-19 in hospital personnel dedicated to patients care with COVID-19 disease A pragmatic multicenter, randomized, double-blind, placebo-controlled trial (CARR-COV-02), International Journal of General Medicine, doi:10.2147/IJGM.S328486.
Gbinigie et al., Platform adaptive trial of novel antivirals for early treatment of COVID-19 In the community (PANORAMIC): protocol for a randomised, controlled, open-label, adaptive platform trial of community novel antiviral treatment of COVID-19 in people at increased risk of more severe disease, BMJ Open, doi:10.1136/bmjopen-2022-069176.
fiercepharma.com, www.fiercepharma.com/pharma/icer-says-pfizers-paxlovid-mercks-molnupiravir-both-cost-effective-drugs-benefit-far-equal.
Butler et al., Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): an open-label, platform-adaptive randomised controlled trial, The Lancet, doi:10.1016/S0140-6736(22)02597-1.
Henderson, J., Ivermectin Arm of PRINCIPLE Trial Put on Hold — Trial website cites supply issues, MedPage Today, www.medpagetoday.com/special-reports/exclusives/96194.
web.archive.org (F), web.archive.org/web/20220104000601/https://www.theepochtimes.com/mkt_app/no-supply-issues-with-ivermectin-pharmaceutical-supplying-principle-oxford-trial_4177066.html.
dailymed.nlm.nih.gov, dailymed.nlm.nih.gov/dailymed/getFile.cfm?setid=847a1dd7-d65b-4a0e-a67d-d90392059dac&type=pdf.
web.archive.org (I), web.archive.org/web/20220104000601/https://www.theepochtimes.com/mkt_app/no-supply-issues-with-ivermectin-pharmaceutical-supplying-principle-oxford-trial_4177066.html.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
principletrial.org (B), www.principletrial.org/news/principle-trial-suspends-hydroxychloroquine-continues-with-focus-on-azithromycin-and-other-drugs.
nihr.ac.uk, www.nihr.ac.uk/news/principle-trial-finds-no-benefit-from-antibiotics-azithromycin-and-doxycycline-for-covid-19-patients/26680.
principletrial.org (C), www.principletrial.org/news/asthma-drug-budesonide-shortens-recovery-time-in-non-hospitalised-patients-with-covid-19.
england.nhs.uk, www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2023/07/COVID-THERAPEUTICS-WEEKLY-PUBLICATION-week-ending-020723-V2.0-OCT-22-Onwards.xlsx.
Behzad et al., Real world Effectiveness of Sotrovimab in Preventing COVID-19–related Hospitalisation or Death in Patients Infected with Omicron BA.2, Journal of Infection and Public Health, doi:10.1016/j.jiph.2023.11.029.
De Vito et al., What Is the Efficacy of Sotrovimab in Reducing Disease Progression and Death in People with COVID-19 during the Omicron Era? Answers from a Real-Life Study, Viruses, doi:10.3390/v15081757.
ox.ac.uk, www.ox.ac.uk/news/2021-04-12-asthma-drug-budesonide-shortens-recovery-time-non-hospitalised-patients-covid-19.
webcache.googleusercontent.com, webcache.googleusercontent.com/search?q=cache:xaz8W3zZ0TgJ:https://rfs2.healthbureau.gov.hk/images/jsn_is_thumbs/images/past_event/Health_Research_Symposium_2021/Materials/HRS2021_K1_powepoint.pdf&hl=en&gl=ie.
Lindsell et al., ACTIV-6: Operationalizing a decentralized, outpatient randomized platform trial to evaluate efficacy of repurposed medicines for COVID-19, Journal of Clinical and Translational Science, doi:10.1017/cts.2023.644.
hra.nhs.uk, www.hra.nhs.uk/planning-and-improving-research/application-summaries/research-summaries/principle-covid-19-uph/.
Moustgaard et al., Impact of blinding on estimated treatment effects in randomised clinical trials: meta-epidemiological study, BMJ, doi:10.1136/bmj.l6802.
reddit.com, www.reddit.com/r/ivermectin/comments/p3vrrt/together_trial_was_not_randomized_possible/.
ufmg.br, ufmg.br/comunicacao/noticias/minas-sao-muitas-distribuicao-de-variantes-do-sars-cov-2-pelo-estado-e-heterogenea.
Sabino et al., Resurgence of COVID-19 in Manaus, Brazil, despite high seroprevalence, Lancet, doi:10.1016/S0140-6736(21)00183-5.
otempo.com.br, www.otempo.com.br/interessa/venda-de-ivermectina-aumenta-nove-vezes-em-minas-e-preocupa-por-risco-a-saude-1.2466432.
odysee.com, odysee.com/@FrontlineCovid19CriticalCareAlliance:c/outpatients-defeating-the-delta-variant:a.
longhaulwiki.com, longhaulwiki.com/resources/assets/Numerous%20issues%20with%20the%20TOGETHER%20trial.pdf.
trialsitenews.com (C), trialsitenews.com/nejm-reported-3-30-that-ivermectin-in-the-together-trial-failed-to-show-significant-benefit-lets-take-a-closer-look/.
covid19criticalcare.com, covid19criticalcare.com/wp-content/uploads/2022/03/Statement-on-Together-Trial-WSJ-Article-Mar-18-1.pdf.
doyourownresearch.substack.com (B), doyourownresearch.substack.com/p/what-went-wrong-with-the-together.
web.archive.org (M), web.archive.org/web/*/https://twitter.com/Covid19Crusher/status/1426612910579757059.
web.archive.org (N), web.archive.org/web/*/https://twitter.com/Covid19Crusher/status/1427255119800848386.
Marinos, A., The Problem With The TOGETHER Trial, doyourownresearch.substack.com/p/the-problem-with-the-together-trial.
Marinos (B), A., TOGETHER Trial: Solving the 3-Day Placebo Subgroup Riddle, doyourownresearch.substack.com/p/the-problem-with-the-together-trial.
doyourownresearch.substack.com (C), doyourownresearch.substack.com/p/the-together-files-1-the-andrew-hill.
doyourownresearch.substack.com (D), doyourownresearch.substack.com/p/together-trial-solving-the-3-day/comment/6143361.
doyourownresearch.substack.com (E), doyourownresearch.substack.com/p/together-trial-impossible-numbers.
doyourownresearch.substack.com (F), doyourownresearch.substack.com/p/demonstrating-randomization-failure.
odysee.com (B), odysee.com/@FrontlineCovid19CriticalCareAlliance:c/weekly_webinar_6April2022:c?t=2507.
Scheim (F) et al., When Characteristics of Clinical Trials Require Per-Protocol as Well as Intention-to-Treat Outcomes to Draw Reliable Conclusions: Three Examples, Journal of Clinical Medicine, doi:10.3390/jcm12113625.
Thorlund et al., Making Statistical Sense of the Molnupiravir MOVe-OUT Clinical Trial, The American Journal of Tropical Medicine and Hygiene, doi:10.4269/ajtmh.21-1339.
Harper, P., Professor tied to altered Andrew Hill paper also prepared 'Ivermectin Evidence' for World Health Organisation, philharper.substack.com/p/professor-tied-to-altered-andrew?s=r.
doyourownresearch.substack.com (G), doyourownresearch.substack.com/p/together-trial-solving-the-3-day.
doyourownresearch.substack.com (H), doyourownresearch.substack.com/p/did-the-placebo-group-in-the-together.
clinicaltrials.gov (C), clinicaltrials.gov/ct2/history/NCT04727424?A=1&B=2&C=Side-by-Side#StudyPageTop.
togethertrial.com (C), www.togethertrial.com/s/EN-Protocol_research_COVID19_AMB_02_Brazil_v10_17Dec2020.pdf.
doyourownresearch.substack.com (I), doyourownresearch.substack.com/p/together-trial-and-the-negative-number.
doyourownresearch.substack.com (J), doyourownresearch.substack.com/p/did-the-together-trial-lie-to-reuters.
ir.eigerbio.com, ir.eigerbio.com/news-releases/news-release-details/eiger-biopharmaceuticals-provides-update-plans-emergency-use.
doyourownresearch.substack.com (K), doyourownresearch.substack.com/p/together-trial-on-ivermectin-did.
doyourownresearch.substack.com (L), doyourownresearch.substack.com/p/when-did-the-ivermectin-and-fluvoxamine.
Lim et al., Efficacy of Ivermectin Treatment on Disease Progression Among Adults With Mild to Moderate COVID-19 and Comorbidities: The I-TECH Randomized Clinical Trial, JAMA, doi:10.1001/jamainternmed.2022.0189.
Forrest et al., Resilient Clinical Trial Infrastructure in Response to the COVID-19 Pandemic: Lessons Learned from the TOGETHER Randomized Platform Clinical Trial, The American Journal of Tropical Medicine and Hygiene, doi:10.4269/ajtmh.21-1202.
doyourownresearch.substack.com (M), doyourownresearch.substack.com/p/was-the-data-in-the-together-trial/comment/6409395.
doyourownresearch.substack.com (N), doyourownresearch.substack.com/p/the-problem-with-the-together-trial/comment/6043250.
doyourownresearch.substack.com (O), doyourownresearch.substack.com/p/the-together-trial-cant-make-up-its?utm_source=twitter&sd=fs&s=r.
cytel.com, www.cytel.com/blog/the-together-trial-cytel-designs-and-implements-novel-adaptive-platform-trial-for-covid-19-therapies.
cytel.com (C), www.cytel.com/news/nordic-capital-and-astorg-invest-in-pharmaceutical-technology-and-advanced-analytics-company-cytel.
empendium.com, empendium.com/mcmtextbook/interviews/perspective/236226%2Ccovid-19-to-treat-or-not-to-treat-platform-trials.
odysee.com (C), odysee.com/@FrontlineCovid19CriticalCareAlliance:c/weekly_webinar_6April2022:c?t=612.
certara.com, www.certara.com/pressrelease/pfizer-deploys-certaras-d360-for-scientific-data-access-and-analysis/.
mmsholdings.com, www.mmsholdings.com/pfizer-selects-mms-as-preferred-provider-for-plain-language-summary-writing-support/.
pierrekory.substack.com (B), pierrekory.substack.com/p/the-false-sinister-and-duplicitous?utm_source=twitter&sd=fs&s=r.
static1.squarespace.com, static1.squarespace.com/static/6112a257d1c1153666ccb987/t/622282bf613a7d79403e7efe/1646428864052/Together_MP_V2.0_25Mar2021.pdf.
static1.squarespace.com (B), static1.squarespace.com/static/6112a257d1c1153666ccb987/t/622283c2cf74fa66a07f6904/1646429124965/Together_MP_V3.0_22June2021.pdf.
Reis (B) et al., Effect of early treatment with fluvoxamine on risk of emergency care and hospitalisation among patients with COVID-19: the TOGETHER randomised, platform clinical trial, The Lancet Global Health, doi:10.1016/S2214-109X(21)00448-4.
Naggie (B) et al., Effect of Higher-Dose Ivermectin for 6 Days vs Placebo on Time to Sustained Recovery in Outpatients With COVID-19: A Randomized Clinical Trial, JAMA, doi:10.1001/jama.2023.1650.
rethinkingclinicaltrials.org, rethinkingclinicaltrials.org/news/grand-rounds-july-22-2022-activ-6-1-year-later-and-trial-results-for-ivermectin-400-and-inhaled-fluticasone-susanna-naggie-md-mhs/.
trialsitenews.com (D), www.trialsitenews.com/a/activ-6-ivermectin-trial-what-really-happened-and-was-the-delta-patient-cohort-under-dosed-a547bb96.
clinicaltrials.gov (F), clinicaltrials.gov/study/NCT05894538?cond=Covid19&intr=ivermectin&page=2&rank=11&tab=results#participant-flow.
Naggie (C), S., Error in the Exclusion of Participants From Analysis in the ACTIV-6 Platform Randomized Clinical Trial, JAMA, doi:10.1001/jama.2024.8723.
doyourownresearch.substack.com (P), doyourownresearch.substack.com/p/activ-6-trial-ivermectin-scientists.
doyourownresearch.substack.com (Q), doyourownresearch.substack.com/p/activ-6-dosing-and-timing-a-fox-in.
doyourownresearch.substack.com (R), doyourownresearch.substack.com/p/the-story-of-a-real-activ-6-patient.
trialsitenews.com (E), www.trialsitenews.com/a/controversial-ivermectin-researcher-failed-to-report-massive-conflict-of-interest.
trialsitenews.com (F), www.trialsitenews.com/a/grotesque-conflicts-of-interest-on-nih-ivermectin-non-recommendation.
doyourownresearch.substack.com (S), doyourownresearch.substack.com/p/activ-6-and-together-bear-strangely.
Wohl et al., Engaging communities in therapeutics clinical research during pandemics: Experiences and lessons from the ACTIV COVID-19 therapeutics research initiative, Journal of Clinical and Translational Science, doi:10.1017/cts.2024.561.
Lindsell (B) et al., The statistical design and analysis of pandemic platform trials: Implications for the future, Journal of Clinical and Translational Science, doi:10.1017/cts.2024.514.
classic.clinicaltrials.gov, classic.clinicaltrials.gov/ct2/history/NCT04510194?A=15&B=16&C=merged#StudyPageTop.
classic.clinicaltrials.gov (B), classic.clinicaltrials.gov/ct2/history/NCT04510194?A=18&B=19&C=merged#StudyPageTop.
rethinkingclinicaltrials.org (B), rethinkingclinicaltrials.org/event/grand-rounds-july-8-results-from-the-covid-out-trial-a-phase-3-trial-of-outpatient-treatment-for-covid-19-using-metformin-ivermectin-and-fluvoxamine/.
trialsitenews.com (G), trialsitenews.com/jama-ivermectin-study-deceived-participants-on-study-drug/.
trialsitenews.com (H), trialsitenews.com/jama-unable-to-confirm-ivermectin-study-consent-form-used-ivermectin/.
trialsitenews.com (I), trialsitenews.com/jama-ivermectin-study-deception-of-study-participants-is-publicly-confirmed/.
francesoir.fr, www.francesoir.fr/societe-sante/la-tromperie-de-letude-jama-sur-livermectine-des-participants-letude-est-confirmee.
trialsitenews.com (J), trialsitenews.com/is-there-a-problem-with-the-lopez-medina-colombia-based-study-implicating-ivermectin-major-pharma-companies-including-merck-funding-the-trial-site-during-the-study/.
web.archive.org (P), web.archive.org/web/*/https://twitter.com/Covid19Crusher/status/1365420061859717124.
scidev.net, www.scidev.net/america-latina/news/uso-excesivo-de-ivermectina-dificulta-saber-si-sirve-contra-covid-19/.
trialsitenews.com (K), trialsitenews.com/ivercovid19-study-in-argentina-disappoints-study-underdoses-ivermectin-comes-up-short/.
Guzman et al., Factors associated with increased mortality in critically ill COVID-19 patients in a Mexican public hospital: the other faces of health system oversaturation, medRxiv, doi:10.1101/2021.03.04.21252084.
web.archive.org (Q), web.archive.org/web/20210917213509/https://twitter.com/jjchamie/status/1438631284163715074.
Butler (B) et al., Doxycycline for community treatment of suspected COVID-19 in people at high risk of adverse outcomes in the UK (PRINCIPLE): a randomised, controlled, open-label, adaptive platform trial, The Lancet Respiratory Medicine, doi:10.1016/S2213-2600(21)00310-6.
Popp et al., Ivermectin for preventing and treating COVID-19, Cochrane Database of Systematic Reviews, doi:10.1002/14651858.CD015017.pub3.
Osati et al., Clinical manifestations and mortality among hospitalized COVID-19 patients in Tanzania, 2021-2022., medRxiv, doi:10.1101/2023.07.13.23292643.
Llenas-García et al., Ivermectin Effect on In-Hospital Mortality and Need for Respiratory Support in COVID-19 Pneumonia: Propensity Score-Matched Retrospective Study, Viruses, doi:10.3390/v15051138.
Wada et al., Efficacy and safety of single-dose ivermectin in mild-to-moderate COVID-19: the double-blind, randomized, placebo-controlled CORVETTE-01 trial, Frontiers in Medicine, doi:10.3389/fmed.2023.1139046.
Munir et al., Clinical Disease Characteristics and Treatment Trajectories Associated with Mortality among COVID-19 Patients in Punjab, Pakistan, Healthcare, doi:10.3390/healthcare11081192.
Desort-Henin et al., The SAIVE Trial, Post-Exposure use of ivermectin in Covid-19 prevention: Efficacy and Safety Results, ECCMID 2023 (results released 1/5/2023), www.medincell.com/wp-content/uploads/2024/03/Poster-SAIVE-April2023-OK3.pdf.
Sarojvisut et al., An Open Label Randomized Controlled Trial of Ivermectin Plus Favipiravir-Based Standard of Care versus Favipiravir-Based Standard of Care for Treatment of Moderate COVID-19 in Thailand, Infection & Chemotherapy, doi:10.3947/ic.2022.0127.
Ochoa-Jaramillo et al., Clinical efficacy and safety of ivermectin (400 μg/kg, single dose) in patients with severe COVID-19: a randomized clinical trial, Revista Infectio, doi:10.22354/24223794.1105.
Mirahmadizadeh et al., Efficacy of single-dose and double-dose ivermectin early treatment in preventing progression to hospitalization in mild COVID-19: A multi-arm, parallel-group randomized, double-blind, placebo-controlled trial, Respirology, doi:10.1111/resp.14318.
Jamir et al., Determinants of Outcome Among Critically Ill Police Personnel With COVID-19: A Retrospective Observational Study From Andhra Pradesh, India, Cureus, doi:10.7759/cureus.20394.
Sweeting et al., What to add to nothing? Use and avoidance of continuity corrections in meta-analysis of sparse data, Statistics in Medicine, doi:10.1002/sim.1761.
Ozer et al., Effectiveness and Safety of Ivermectin in COVID-19 Patients: A Prospective Study at A Safety-Net Hospital, Journal of Medical Virology, doi:10.1002/jmv.27469.
Morgenstern (B) et al., The Use of Compassionate Ivermectin in the Management of Symptomatic Outpatients and Hospitalized Patients with Clinical Diagnosis of Covid-19 at the Centro Medico Bournigal and at the Centro Medico Punta Cana, Grupo Rescue, Dominican Republic, from May 1 to August 10, 2020, J. Clinical Trials (preprint 11/3), www.longdom.org/open-access/the-use-of-compassionate-ivermectin-in-the-management-of-symptomatic-outpatients-and-hospitalized-patients-with-clinical.pdf.
Vallejos (B) et al., Ivermectina en agentes de salud e ivercor COVID-19: resultados al 18 de feb 2021, web.archive.org/web/*/https://twitter.com/Covid19Crusher/status/1365420061859717124.
Mateja et al., The choice of viral load endpoint in early phase trials of COVID-19 treatments aiming to reduce 28-day hospitalization and/or death, The Journal of Infectious Diseases, doi:10.1093/infdis/jiaf282.
Zhang (C) et al., What's the relative risk? A method of correcting the odds ratio in cohort studies of common outcomes, JAMA, 80:19, 1690, doi:10.1001/jama.280.19.1690.
Altman (B) et al., How to obtain the confidence interval from a P value, BMJ, doi:10.1136/bmj.d2090.
Kamal et al., Ivermectin In Treatment of COVID 19 Patients, NCT04425707, clinicaltrials.gov/study/NCT04425707.
Please send us corrections, updates, or comments.
c19early involves the extraction of 200,000+ datapoints from
thousands of papers. Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation. IMA and WCH
provide treatment protocols.