Pharmacometrics of high dose ivermectin in early COVID-19: an open label, randomized, controlled adaptive platform trial (PLATCOV)
William Hk Schilling, Podjanee Jittamala, James A Watson, Maneerat Ekkapongpisit, Tanaya Siripoon, Thundon Ngamprasertchai, Viravarn Luvira, Sasithorn Pongwilai, Cintia Cruz, James J Callery, Simon Boyd, Varaporn Kruabkontho, Thatsanun Ngernseng, Jaruwan Tubprasert, Mohammad Yazid Abdad, Nattaporn Piaraksa, Kanokon Suwannasin, Pongtorn Hanboonkunupakarn, Borimas Hanboonkunupakarn, Sakol Sookprome, Kittiyod Poovorawan, Janjira Thaipadungpanit, Stuart Blacksell, Mallika Imwong, Joel Tarning, Walter Rj Taylor, Vasin Chotivanich, Chunlanee Sangketchon, Wiroj Ruksakul, Kesinee Chotivanich, Mauro M Teixeira, Sasithon Pukrittayakamee, Arjen M Dondorp, Nicholas Pj Day, Watcharapong Piyaphanee, Weerapong Phumratanaprapin, Nicholas J White
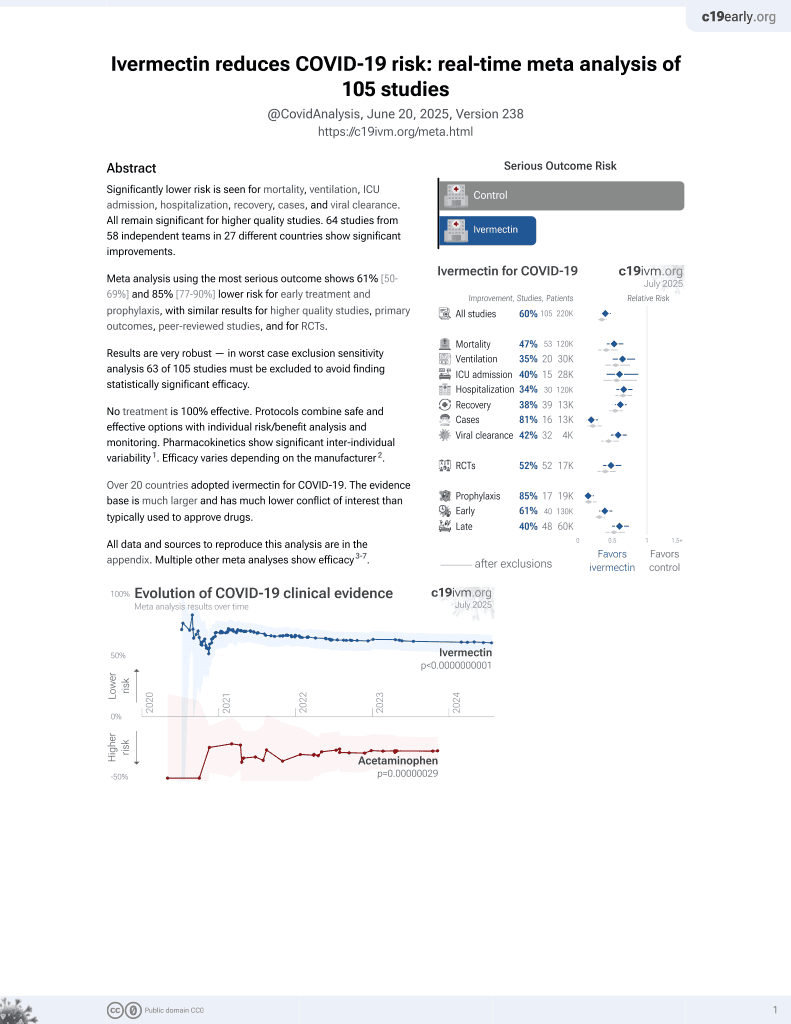
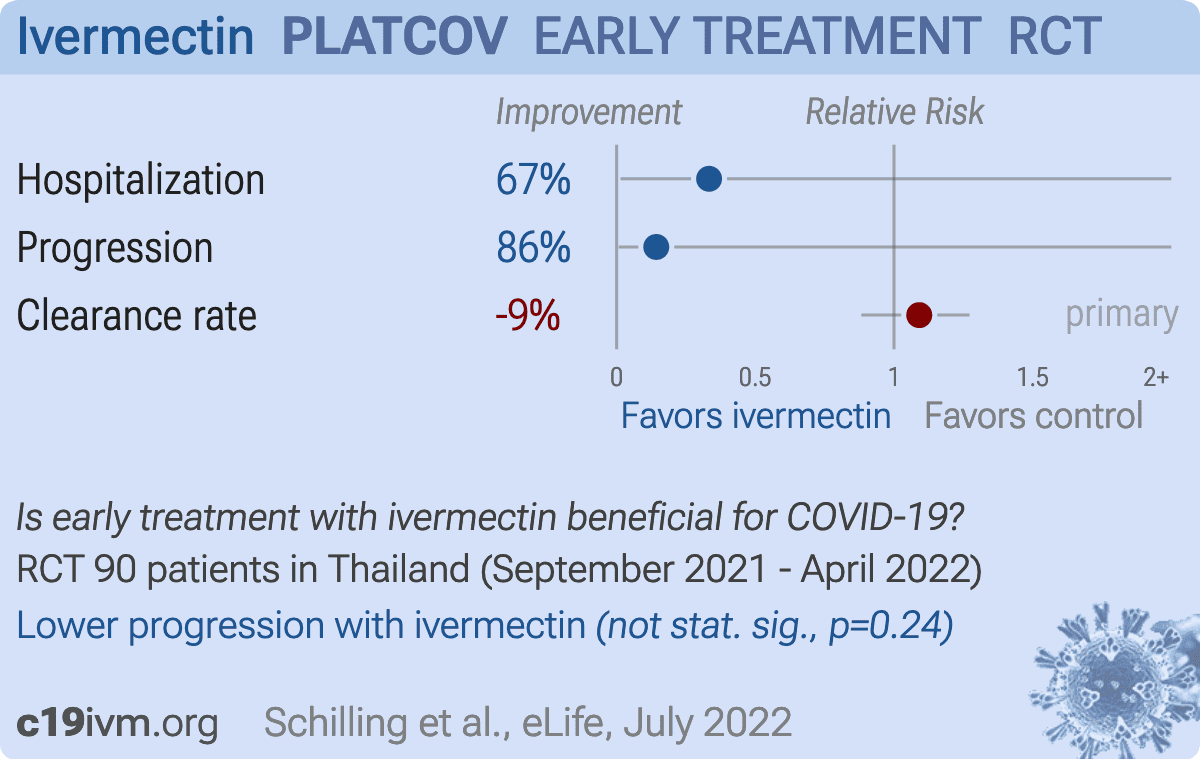
High dose ivermectin did not have measurable antiviral activity in early symptomatic COVID-19. Pharmacometric evaluation of viral clearance rates based on frequent oropharyngeal sampling is a highly efficient and well-tolerated method of assessing and comparing SARS CoV-2 antiviral therapeutics in vivo.
Identifications were confirmed using Whole Genome Sequencing as below: The sequencing method carried out in this experiment follows the "PCR tiling of SARS-CoV-2 virus with rapid barcoding and Midnight RT PCR Expansion" provided by Oxford Nanopore Technology (Oxford, UK) developed based on a protocol by ARTIC network group 1 . Library preparation process started with reverse transcription, which consists of mixing the purified viral RNA with LunaScript RT SuperMix and incubating the mixtures in a thermal cycler. DNA fragments to be used in the assembly process were amplified by PCR using Midnight primer set (V3) and attached with barcodes from Rapid Barcode Plate (RB96). The mixtures from each sample were pooled together, cleaned with AMPure XP Beads (AXP) and attached with Rapid Adapter F (RAP F). The prepared DNA fragments were then loaded into a primed flow cell (FLO-MIN106) and sequenced on GridION MK1 system.
Viral genome assembly and classification The output sequencing data (.fast5) from MinKNOW software was base-called with Guppy software using the High Accuracy (HAC) model to generate nucleotide sequence data for each fragment (reads) in the fastq format. These base-called data were then processed through the established workflow wf-artic on EPI2ME software to be assembled into consensus sequences. Only reads with average Phred Quality (Q) score above 9 and Adverse events (AE) and Serious Adverse Events See supplementary files for: Supplementary file..
References
Bernal, Da Silva, Musungaie, Molnupiravir for Oral Treatment of Covid-19 in Nonhospitalized Patients, N Engl J Med
Bruel, Hadjadj, Maes, Serum neutralization of SARS-CoV-2 Omicron sublineages BA.1 and BA.2 in patients receiving monoclonal antibodies, Nat Med
Caly, Druce, Catton, Jans, Wagstaff, The FDA-approved drug ivermectin inhibits the replication of SARS-CoV-2 in vitro, Antiviral Res
Gottlieb, Vaca, Paredes, Early Remdesivir to Prevent Progression to Severe Covid-19 in Outpatients, N Engl J Med
Hammond, Leister-Tebbe, Gardner, Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with Covid-19, N Engl J Med
Jittamala, Schilling, Watson, Clinical antiviral efficacy of remdesivir and casirivimab/imdevimab against the SARS-CoV-2 Delta and Omicron variants
Kobylinski, Jittamala, Hanboonkunupakarn, Safety, Pharmacokinetics, and Mosquito-Lethal Effects of Ivermectin in Combination With Dihydroartemisinin-Piperaquine and Primaquine in Healthy Adult Thai Subjects, Clin Pharmacol Ther
Kobylinski, Jittamala, Hanboonkunupakarn, Safety, Pharmacokinetics, and Mosquito-Lethal Effects of Ivermectin in Combination With Dihydroartemisinin-Piperaquine and Primaquine in Healthy Adult Thai Subjects, Clin Pharmacol Ther
Lange, Little, Taylor, Robust Statistical Modeling Using the t Distribution
Lawrence, Meyerowitz-Katz, Heathers, Brown, Sheldrick, The lesson of ivermectin: meta-analyses based on summary data alone are inherently unreliable, Nat Med
Mclean, Rashan, Tran, The fragmented COVID-19 therapeutics research landscape: a living systematic review of clinical trial registrations evaluating priority pharmacological interventions
Mega, Latin America's embrace of an unproven COVID treatment is hindering drug trials, Nature
Munoz-Fontela, Widerspick, Albrecht, Advances and gaps in SARS-CoV-2 infection models, PLoS Pathog
Natori, Alghamdi, Tazari, Use of Viral Load as a Surrogate Marker in Clinical Studies of Cytomegalovirus in Solid Organ Transplantation: A Systematic Review and Meta-analysis, Clin Infect Dis,
doi:10.1093/cid/cix793Navarro, Camprubí, Requena-Méndez, Safety of high-dose ivermectin: a systematic review and meta-analysis, J Antimicrob Chemother
O'brien, Forleo-Neto, Musser, Subcutaneous REGEN-COV Antibody Combination to Prevent Covid-19, N Engl J Med
Reis, Silva, Silva, Effect of Early Treatment with Ivermectin among Patients with Covid-19, N Engl J Med
Rnase, Adjustment, adjustment for site & variant; WIP
Road, Bangkok, Tambon Bang Phli Yai, Amphoe Bangplee
Robinson, Liew, Tanner, COVID-19 therapeutics: Challenges and directions for the future, Proc Natl Acad Sci U S A
Sigal, Milo, Jassat, Estimating disease severity of Omicron and Delta SARS-CoV-2 infections, Nat Rev Immunol
Smit, Ochomo, Aljayyoussi, Safety and mosquitocidal efficacy of highdose ivermectin when co-administered with dihydroartemisinin-piperaquine in Kenyan adults with uncomplicated malaria (IVERMAL): a randomised, double-blind, placebocontrolled trial, Lancet Infect Dis
Tipthara, Kobylinski, Godejohann, Hanboonkunupakarn, Roth et al., Identification of the metabolites of ivermectin in humans, Pharmacol Res Perspect
Watson, Kissler, Day, Grad, White, Characterizing SARS-CoV-2 Viral Clearance Kinetics to Improve the Design of Antiviral Pharmacometric Studies, Antimicrob Agents Chemother
Weinreich, Sivapalasingam, Norton, REGEN-COV Antibody Combination and Outcomes in Outpatients with Covid-19, N Engl J Med
Yu, Liao, Yuan, Effectiveness of oseltamivir on disease progression and viral RNA shedding in patients with mild pandemic 2009 influenza A H1N1: opportunistic retrospective study of medical charts in China, BMJ
DOI record:
{
"DOI": "10.7554/elife.83201",
"ISSN": [
"2050-084X"
],
"URL": "http://dx.doi.org/10.7554/eLife.83201",
"abstract": "<jats:p><jats:bold>Background:</jats:bold> There is no generally accepted methodology for <jats:italic>in vivo</jats:italic> assessment of antiviral activity in SARS-CoV-2 infections. Ivermectin has been recommended widely as a treatment of COVID-19, but whether it has clinically significant antiviral activity <jats:italic>in vivo</jats:italic> is uncertain.</jats:p><jats:p><jats:bold>Methods:</jats:bold> In a multicentre open label, randomized, controlled adaptive platform trial, adult patients with early symptomatic COVID-19 were randomized to one of six treatment arms including high dose oral ivermectin (600µg/kg daily for seven days), the monoclonal antibodies casirivimab and imdevimab (600mg/600mg), and no study drug. The primary outcome was the comparison of viral clearance rates in the modified intention-to-treat population (mITT). This was derived from daily log<jats:sub>10</jats:sub> viral densities in standardized duplicate oropharyngeal swab eluates. This ongoing trial is registered at ClinicalTrials.gov (NCT05041907).</jats:p><jats:p><jats:bold>Results:</jats:bold> Randomization to the ivermectin arm was stopped after enrolling 205 patients into all arms, as the prespecified futility threshold was reached. Following ivermectin the mean estimated rate of SARS-CoV-2 viral clearance was 9.1% slower [95%CI -27.2% to +11.8%; n=45] than in the no drug arm [n=41], whereas in a preliminary analysis of the casirivimab/imdevimab arm it was 52.3% faster [95%CI +7.0% to +115.1%; n=10 (Delta variant) versus n=41].</jats:p><jats:p><jats:bold>Conclusions:</jats:bold> High dose ivermectin did not have measurable antiviral activity in early symptomatic COVID-19. Pharmacometric evaluation of viral clearance rate from frequent serial oropharyngeal qPCR viral density estimates is a highly efficient and well tolerated method of assessing SARS CoV-2 antiviral therapeutics <jats:italic>in vivo</jats:italic>.</jats:p><jats:p><jats:bold>Funding:</jats:bold> 'Finding treatments for COVID-19: A phase 2 multi-centre adaptive platform trial to assess antiviral pharmacodynamics in early symptomatic COVID-19 (PLAT-COV)' is supported by the Wellcome Trust Grant ref: 223195/Z/21/Z through the COVID-19 Therapeutics Accelerator.</jats:p><jats:p><jats:bold>Clinical trial number:</jats:bold> ClinicalTrials.gov (NCT05041907).</jats:p>",
"accepted": {
"date-parts": [
[
2023,
2,
3
]
]
},
"alternative-id": [
"10.7554/eLife.83201"
],
"assertion": [
{
"group": {
"name": "peer_review_taxonomy"
},
"label": "Peer review transparency",
"name": "peer_review_transparency",
"value": "single anonymised"
},
{
"group": {
"name": "peer_review_taxonomy"
},
"label": "Peer review interaction",
"name": "peer_review_interaction",
"value": "other reviewer(s), editor"
},
{
"group": {
"name": "peer_review_taxonomy"
},
"label": "Peer review published",
"name": "peer_review_published",
"value": "review summaries, review reports, author/editor communication, reviewer identities reviewer opt in, editor identities"
},
{
"group": {
"name": "post_publication_commenting"
},
"label": "Post publication commenting",
"name": "post_publication_commenting",
"value": "open (sign in with ORCID iD required)"
}
],
"author": [
{
"ORCID": "http://orcid.org/0000-0002-6328-8748",
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "Schilling",
"given": "William HK",
"sequence": "first"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Jittamala",
"given": "Podjanee",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-5524-0325",
"affiliation": [
{
"name": "Nuffield Department of Medicine, Oxford University Clinical Research Unit",
"place": [
"Oxford, United Kingdom"
]
}
],
"authenticated-orcid": true,
"family": "Watson",
"given": "James A",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Ekkapongpisit",
"given": "Maneerat",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Clinical Tropical Medicine, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Siripoon",
"given": "Tanaya",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Clinical Tropical Medicine, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Ngamprasertchai",
"given": "Thundon",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-9270-3720",
"affiliation": [
{
"name": "Department of Clinical Tropical Medicine, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "Luvira",
"given": "Viravarn",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Pongwilai",
"given": "Sasithorn",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-8393-8536",
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "Cruz",
"given": "Cintia Valeria",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-3218-2166",
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "Callery",
"given": "James J",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Boyd",
"given": "Simon",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Kruabkontho",
"given": "Varaporn",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Ngernseng",
"given": "Thatsanun",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Tubprasert",
"given": "Jaruwan",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Abdad",
"given": "Mohammad Yazid",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Piaraksa",
"given": "Nattaporn",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Suwannasin",
"given": "Kanokon",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Bangplee Hospital, Ministry of Public Health",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Hanboonkunupakarn",
"given": "Pongtorn",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Hanboonkunupakarn",
"given": "Borimas",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Bangplee Hospital, Ministry of Public Health",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Sookprome",
"given": "Sakol",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Poovorawan",
"given": "Kittiyod",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-6184-3381",
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "Thaipadungpanit",
"given": "Janjira",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Blacksell",
"given": "Stuart",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Imwong",
"given": "Mallika",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0003-4566-4030",
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "Tarning",
"given": "Joel",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Taylor",
"given": "Walter RJ",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Faculty of Medicine, Navamindradhiraj University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Chotivanich",
"given": "Vasin",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Faculty of Science and Health Technology, Navamindradhiraj University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Sangketchon",
"given": "Chunlanee",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Faculty of Medicine, Navamindradhiraj University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Ruksakul",
"given": "Wiroj",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Chotivanich",
"given": "Kesinee",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-6944-3008",
"affiliation": [
{
"name": "Department of Biochemistry and Immunology, Universidade Federal de Minas Gerais",
"place": [
"Belo Horizonte, Brazil"
]
}
],
"authenticated-orcid": true,
"family": "Teixeira",
"given": "Mauro Martins",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Pukrittayakamee",
"given": "Sasithon",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0001-5190-2395",
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "Dondorp",
"given": "Arjen M",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0003-2309-1171",
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "Day",
"given": "Nicholas PJ",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Clinical Tropical Medicine, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Piyaphanee",
"given": "Watcharapong",
"sequence": "additional"
},
{
"affiliation": [
{
"name": "Department of Clinical Tropical Medicine, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"family": "Phumratanaprapin",
"given": "Weerapong",
"sequence": "additional"
},
{
"ORCID": "http://orcid.org/0000-0002-1897-1978",
"affiliation": [
{
"name": "Mahidol Oxford Tropical Medicine Research Unit, Mahidol University",
"place": [
"Bangkok, Thailand"
]
}
],
"authenticated-orcid": true,
"family": "White",
"given": "Nicholas J",
"sequence": "additional"
},
{
"affiliation": [],
"name": "on behalf of the PLATCOV Collaborative Group",
"sequence": "additional"
}
],
"container-title": "eLife",
"content-domain": {
"crossmark-restriction": false,
"domain": [
"elifesciences.org"
]
},
"created": {
"date-parts": [
[
2023,
2,
21
]
],
"date-time": "2023-02-21T00:00:54Z",
"timestamp": 1676937654000
},
"deposited": {
"date-parts": [
[
2023,
2,
21
]
],
"date-time": "2023-02-21T00:02:48Z",
"timestamp": 1676937768000
},
"funder": [
{
"DOI": "10.13039/100010269",
"award": [
"223195/Z/21/Z"
],
"doi-asserted-by": "publisher",
"name": "Wellcome Trust"
},
{
"DOI": "10.13039/100010269",
"award": [
"223195/Z/21/Z"
],
"doi-asserted-by": "publisher",
"name": "Wellcome Trust"
},
{
"DOI": "10.13039/100010269",
"award": [
"223195/Z/21/Z"
],
"doi-asserted-by": "publisher",
"name": "Wellcome Trust"
}
],
"indexed": {
"date-parts": [
[
2023,
2,
21
]
],
"date-time": "2023-02-21T05:35:51Z",
"timestamp": 1676957751211
},
"is-referenced-by-count": 0,
"issued": {
"date-parts": [
[
2023,
2,
21
]
]
},
"language": "en",
"license": [
{
"URL": "http://creativecommons.org/licenses/by/4.0/",
"content-version": "vor",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2023,
2,
21
]
],
"date-time": "2023-02-21T00:00:00Z",
"timestamp": 1676937600000
}
},
{
"URL": "http://creativecommons.org/licenses/by/4.0/",
"content-version": "am",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2023,
2,
21
]
],
"date-time": "2023-02-21T00:00:00Z",
"timestamp": 1676937600000
}
},
{
"URL": "http://creativecommons.org/licenses/by/4.0/",
"content-version": "tdm",
"delay-in-days": 0,
"start": {
"date-parts": [
[
2023,
2,
21
]
],
"date-time": "2023-02-21T00:00:00Z",
"timestamp": 1676937600000
}
}
],
"link": [
{
"URL": "https://cdn.elifesciences.org/articles/83201/elife-83201-v1.pdf",
"content-type": "application/pdf",
"content-version": "vor",
"intended-application": "text-mining"
},
{
"URL": "https://cdn.elifesciences.org/articles/83201/elife-83201-v1.xml",
"content-type": "application/xml",
"content-version": "vor",
"intended-application": "text-mining"
}
],
"member": "4374",
"original-title": [],
"prefix": "10.7554",
"published": {
"date-parts": [
[
2023,
2,
21
]
]
},
"published-online": {
"date-parts": [
[
2023,
2,
21
]
]
},
"publisher": "eLife Sciences Publications, Ltd",
"reference-count": 0,
"references-count": 0,
"relation": {
"is-supplemented-by": [
{
"asserted-by": "subject",
"id": "https://github.com/jwatowatson/PLATCOV-Ivermectin",
"id-type": "uri"
}
]
},
"resource": {
"primary": {
"URL": "https://elifesciences.org/articles/83201"
}
},
"score": 1,
"short-title": [],
"source": "Crossref",
"subject": [
"General Immunology and Microbiology",
"General Biochemistry, Genetics and Molecular Biology",
"General Medicine",
"General Neuroscience"
],
"subtitle": [],
"title": "Pharmacometrics of high dose ivermectin in early COVID-19: an open label, randomized, controlled adaptive platform trial (PLATCOV)",
"type": "journal-article",
"update-policy": "http://dx.doi.org/10.7554/elife.83201",
"volume": "12"
}

{kind=link}
{kind=link}