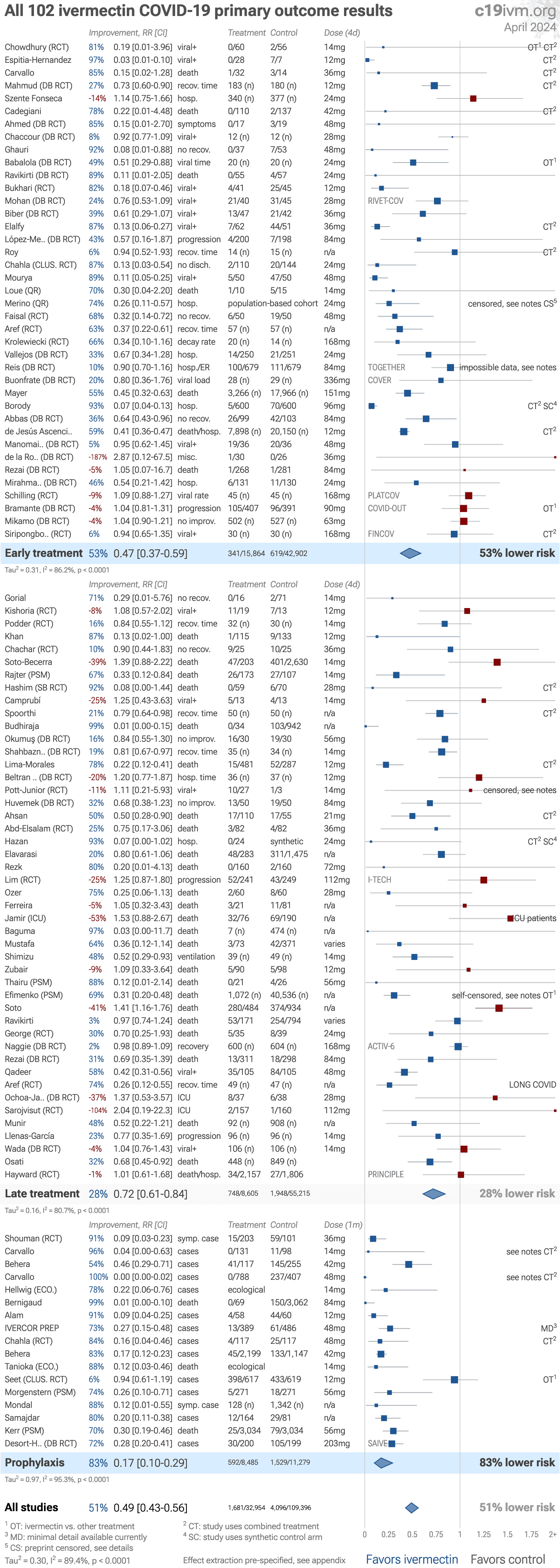
Figure S1. Random effects meta-analysis for
primary outcomes (as defined before the trial started).
Loading..
Figure S2. Random effects meta-analysis for
peer-reviewed studies after exclusions. Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Loading..
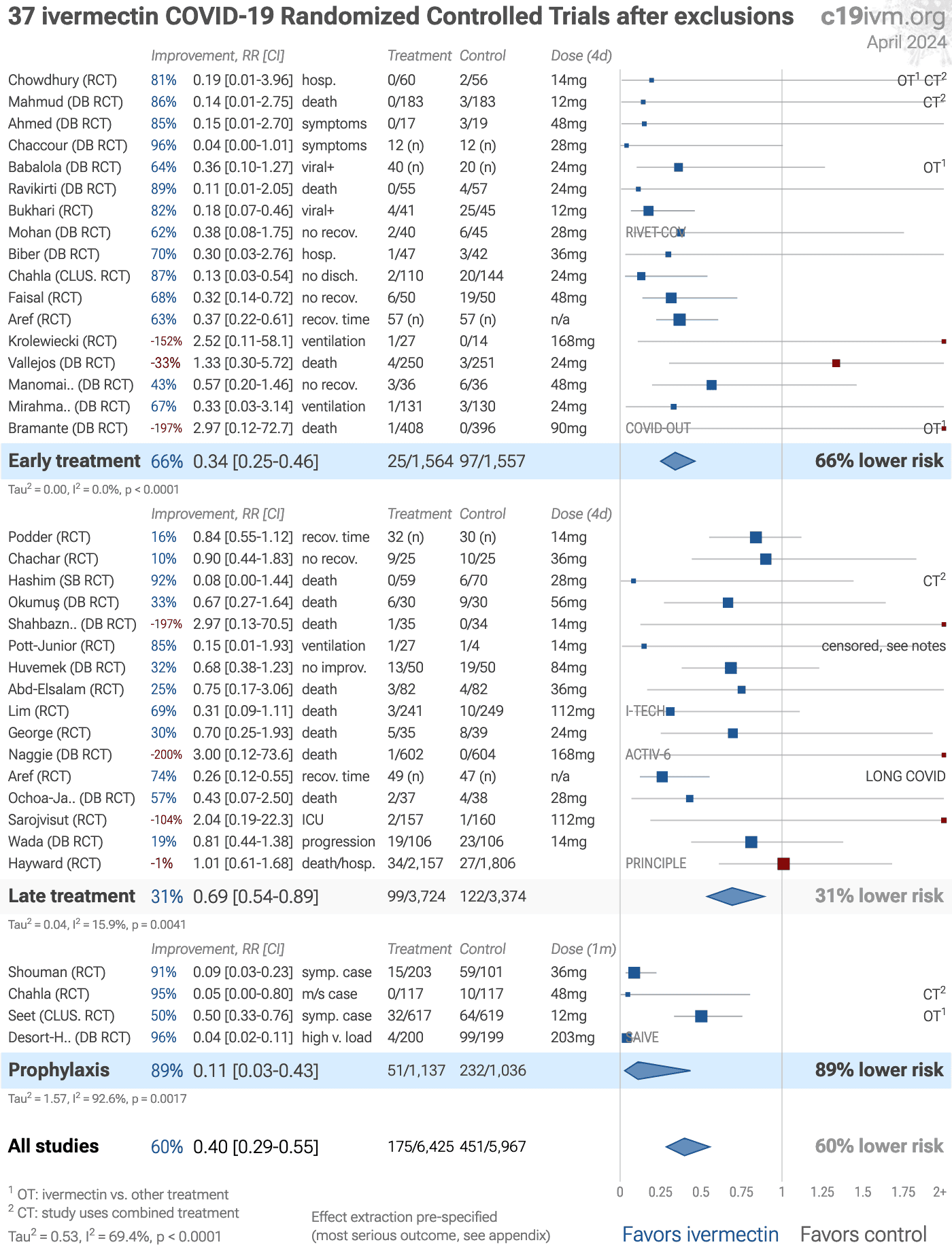
Figure S3. Random effects meta-analysis for
RCT studies after exclusions. Effect extraction is pre-specified, using the most serious outcome reported,
see the appendix for details.
Analysis validating pooled outcomes for
COVID-19 can be found below.
Loading..
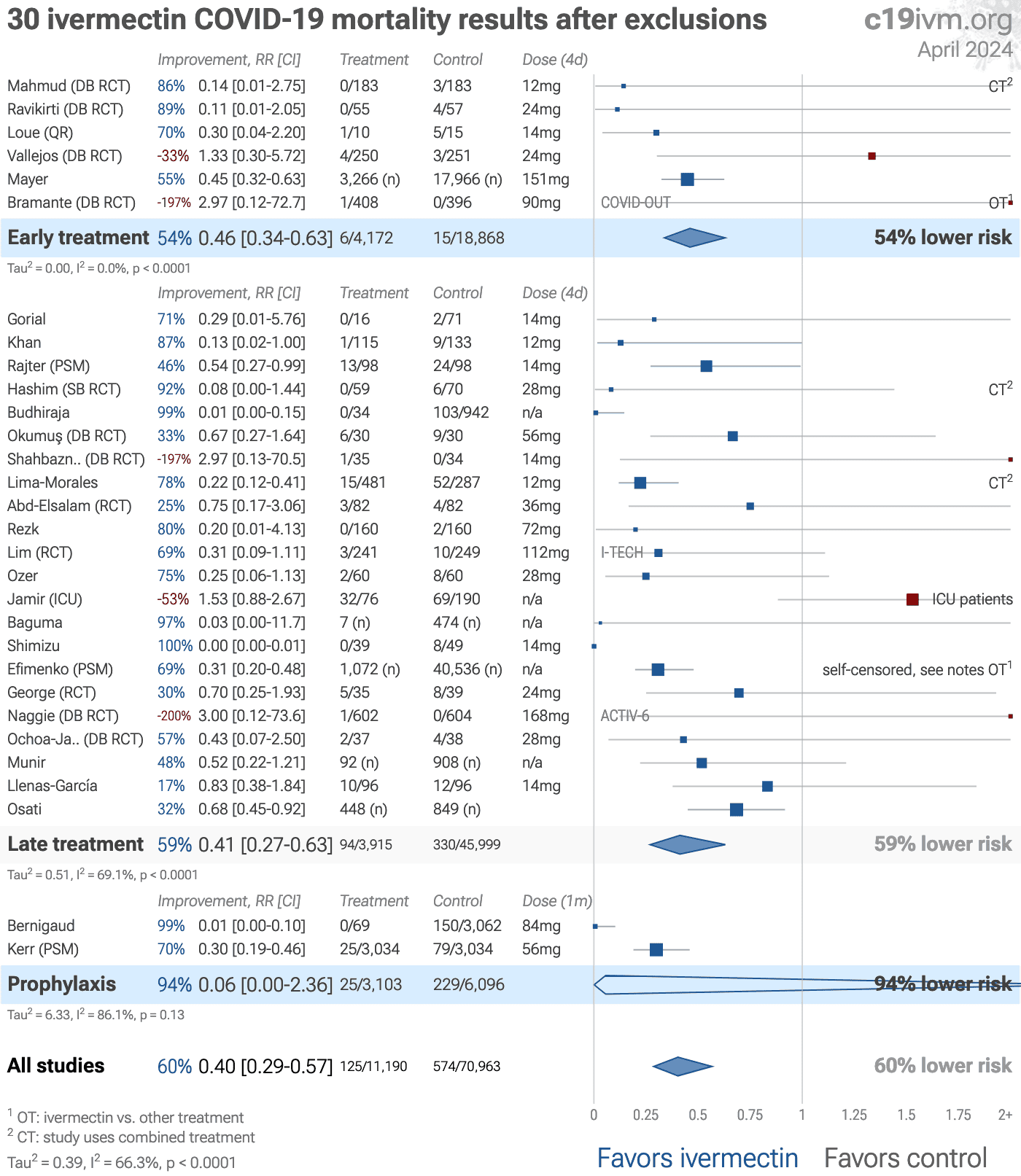
Figure S4. Random effects meta-analysis for
mortality after exclusions.
Loading..
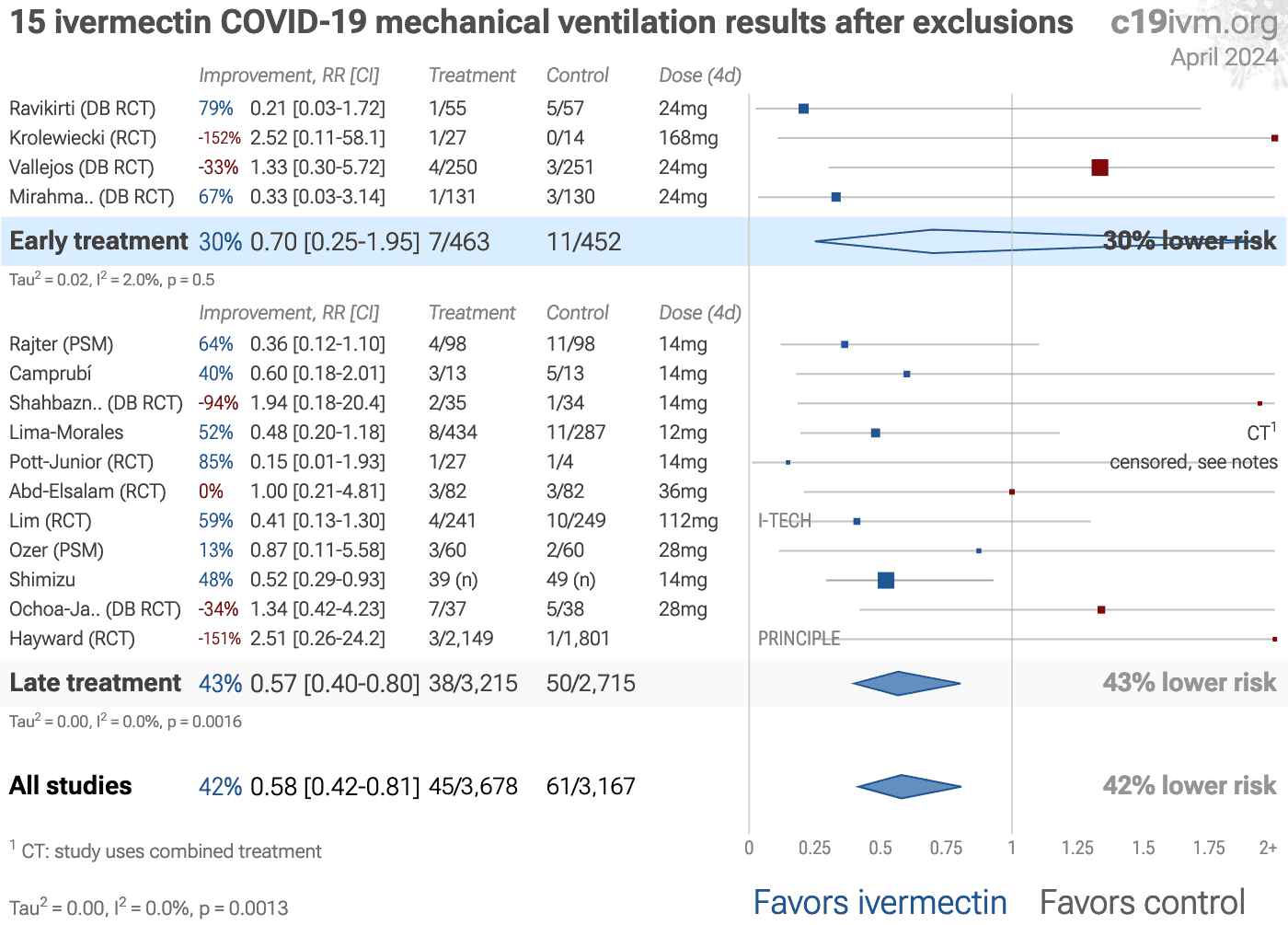
Figure S5. Random effects meta-analysis for
mechanical ventilation after exclusions.
Loading..
Figure S6. Random effects meta-analysis for
ICU admission after exclusions.
Loading..
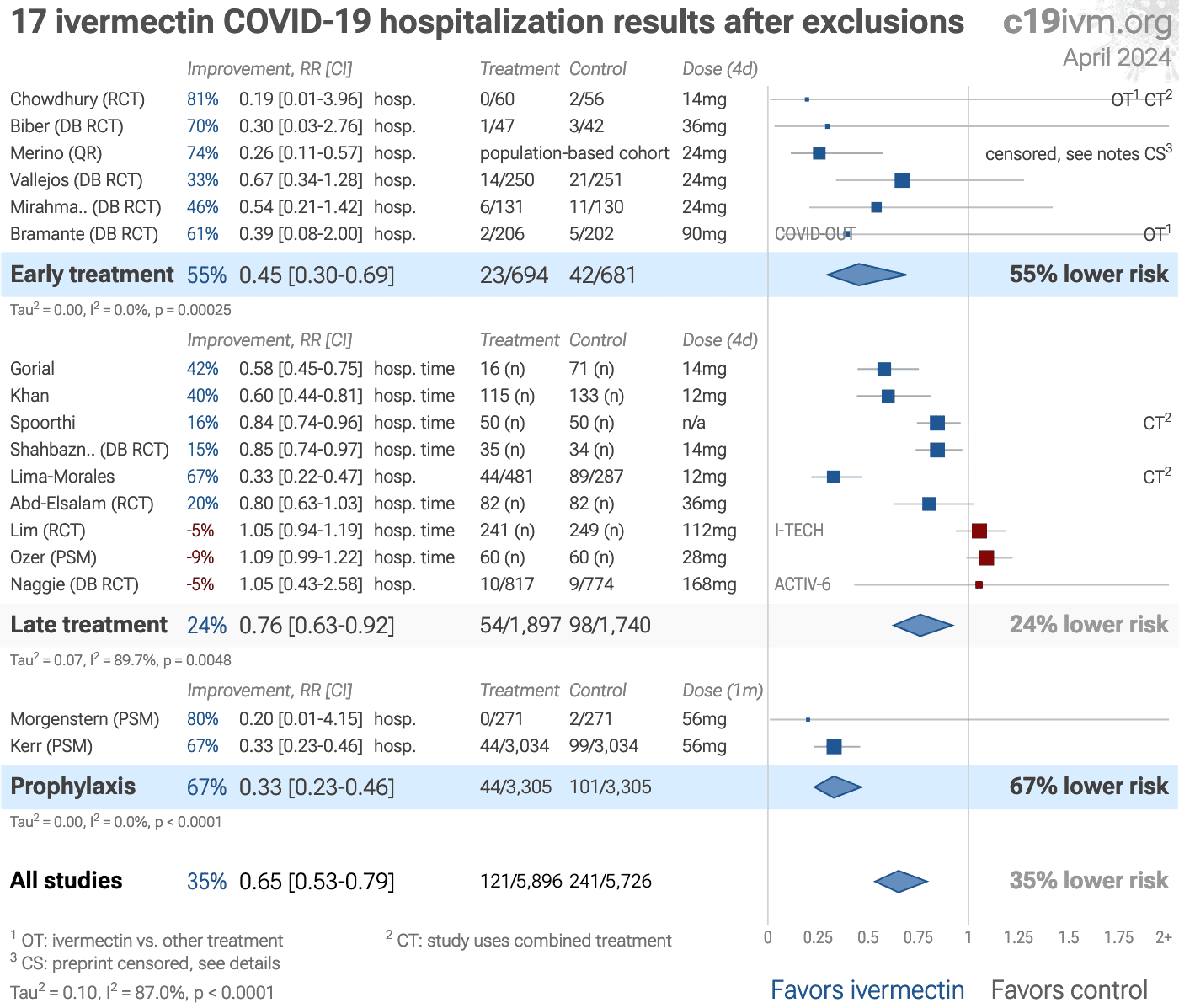
Figure S7. Random effects meta-analysis for
hospitalization after exclusions.
Loading..
Figure S8. Random effects meta-analysis for
recovery results only after exclusions.
Loading..
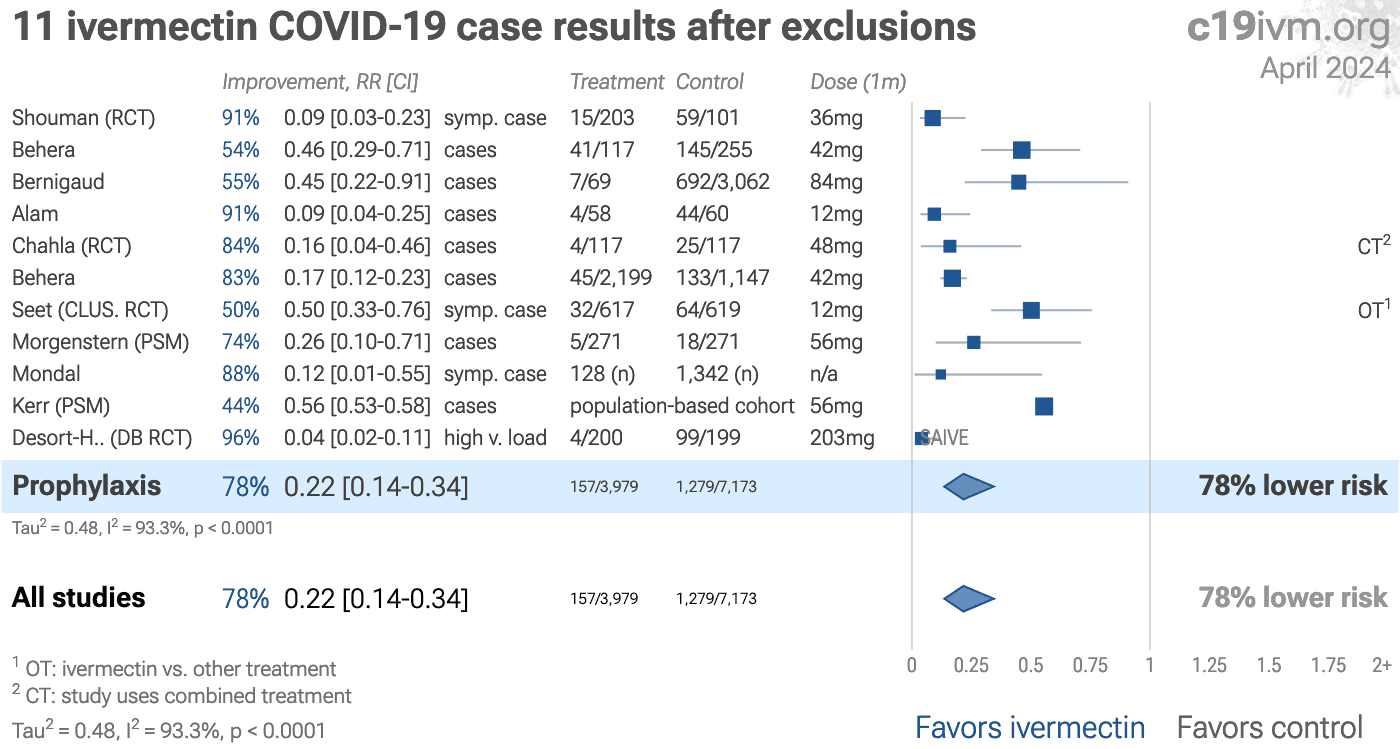
Figure S9. Random effects meta-analysis for
COVID-19 case results after exclusions.
Loading..
Figure S10. Random effects meta-analysis for
viral clearance after exclusions.
Loading..
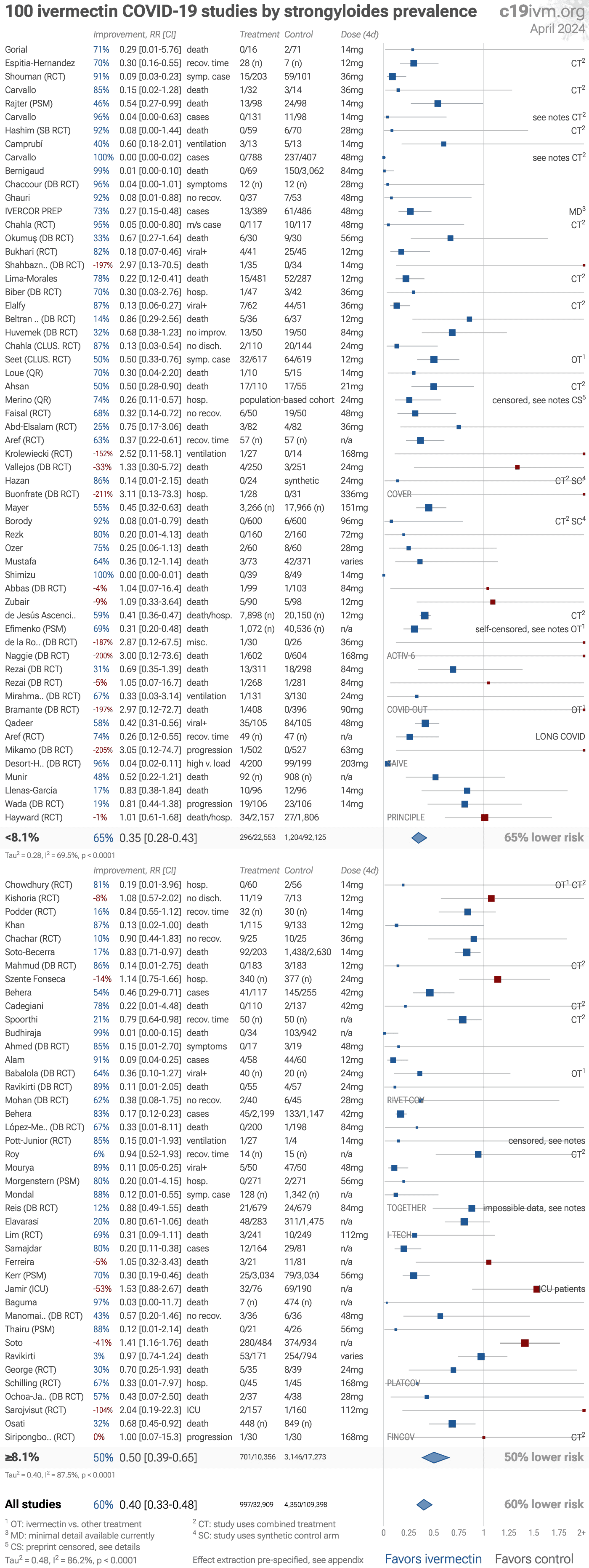
Figure S11. Random effects meta-analysis
for studies grouped by strongyloides prevalence. Data is by
country and from Buonfrate. Effect extraction follows the same
pre-specified protocol as detailed in the appendix.
Loading..
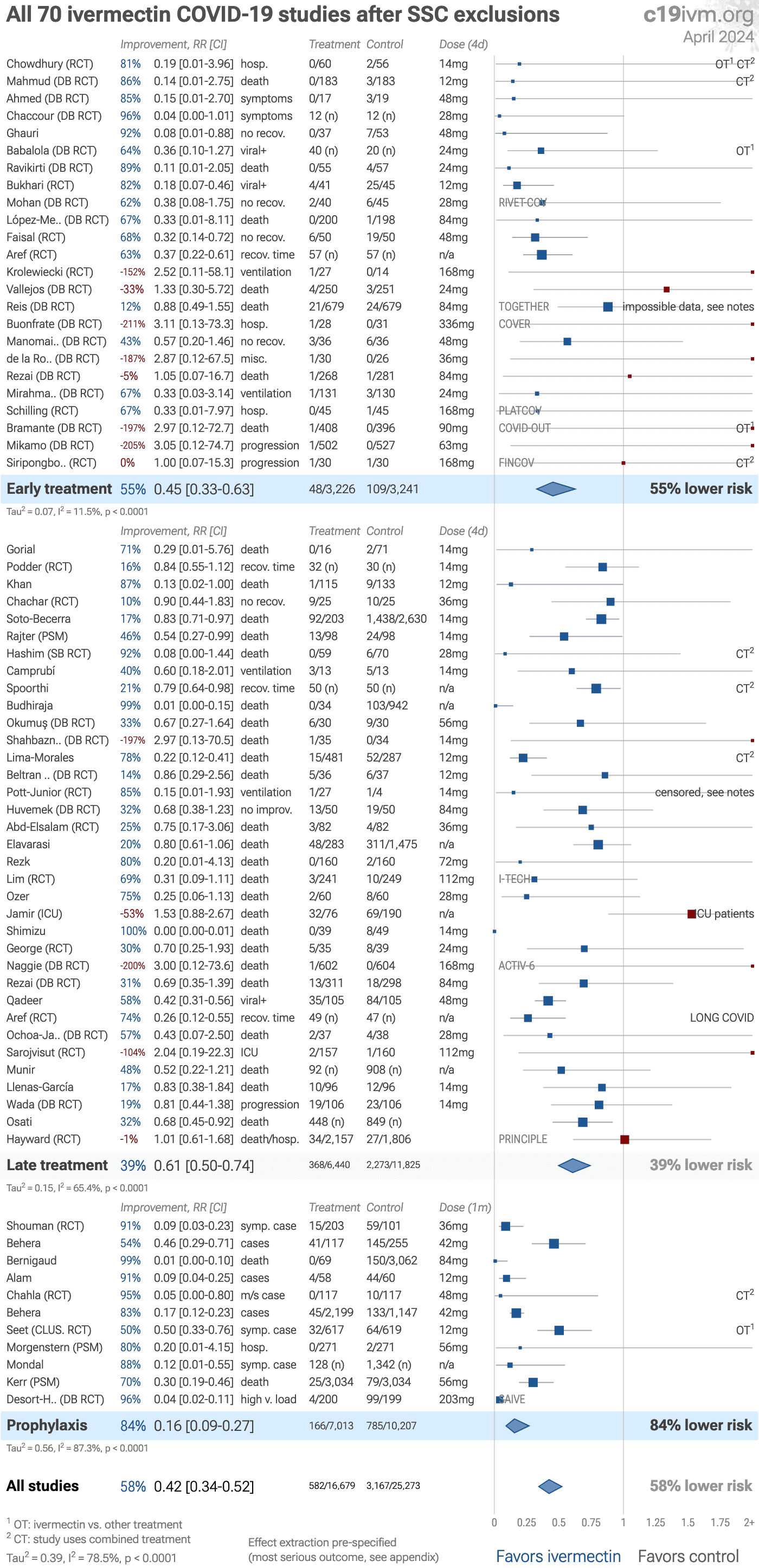
Figure S12. Random effects meta-analysis
with SSC exclusions. SSC has not reviewed late treatment and prophylaxis
trials. SSC exclusions are from Nov 27, 2021.
Loading..
Figure S13. Random effects meta-analysis
with GMK exclusions. Our main exclusion analyses already exclude all studies
where the GMK team believes there are major data issues. This analysis
corresponds with GMK's recommendation for meta analysis as of Oct 26, 2021.
GMK excludes most non-RCT studies, with the notable exception of several
studies with major issues that report negative or relatively poor results
— Szente Fonseca which is likely affected by multicollinearity among
treatments, Elavarasi which reports unadjusted results with no group
details and is subject to confounding by indication, and
Soto-Becerra which has several major issues described in the
details.
Loading..
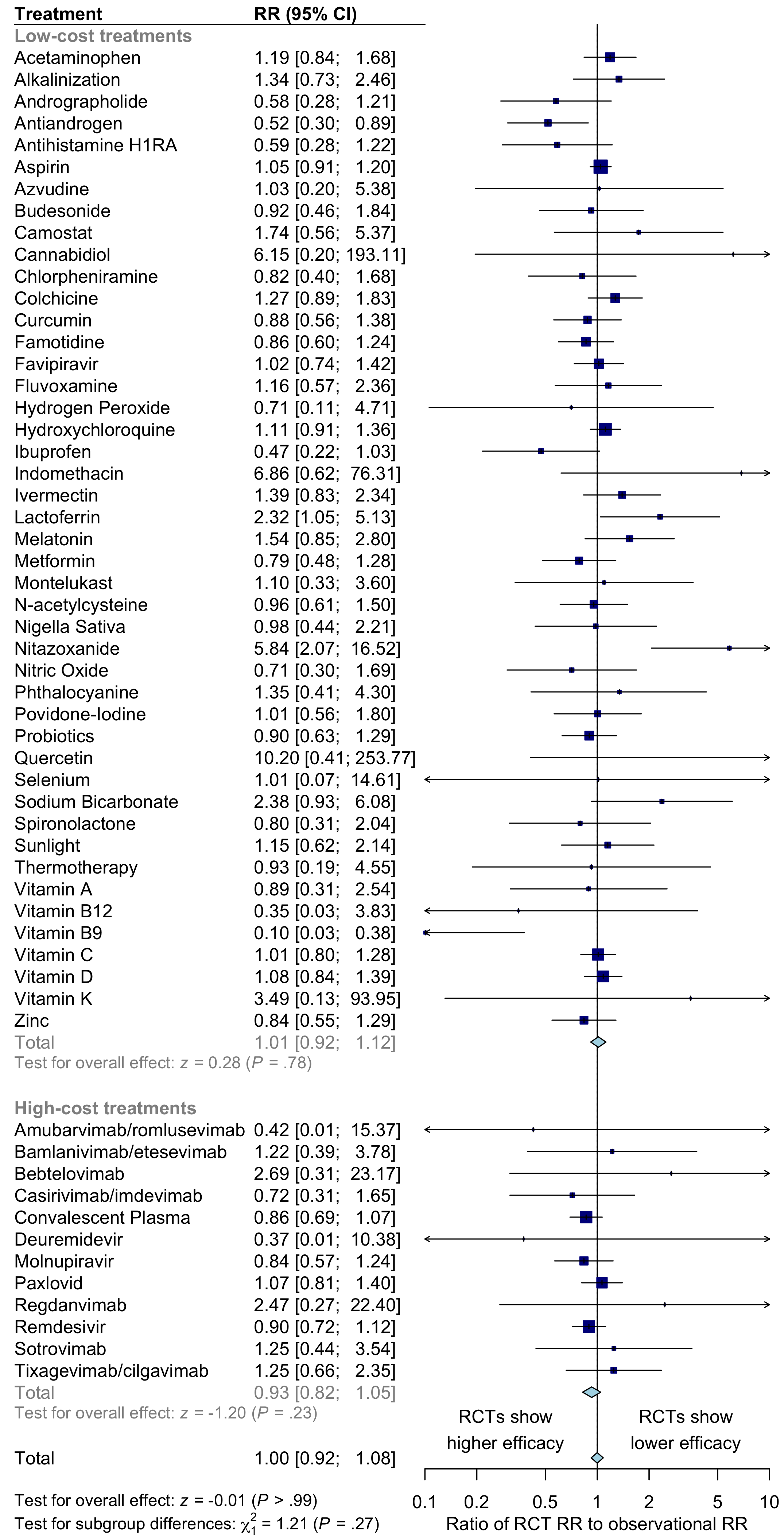
Figure S14. Comparison of results for RCTs versus observational studies. For COVID-19 treatments, there is no significant difference between the results of RCTs and observational studies. Observational studies do not systematically over or underestimate efficacy. For high-cost treatments, there is a non-significant trend towards RCTs showing greater efficacy.
Please send us corrections, updates, or comments.
c19early involves the extraction of 200,000+ datapoints from
thousands of papers. Community updates
help ensure high accuracy.
Treatments and other interventions are complementary.
All practical, effective, and safe
means should be used based on risk/benefit analysis.
No treatment or intervention is 100% available and effective for all current
and future variants.
We do not provide medical advice. Before taking any medication,
consult a qualified physician who can provide personalized advice and details
of risks and benefits based on your medical history and situation. IMA and WCH
provide treatment protocols.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}